Foot Pronation, Supination and Pelvic Floor Health
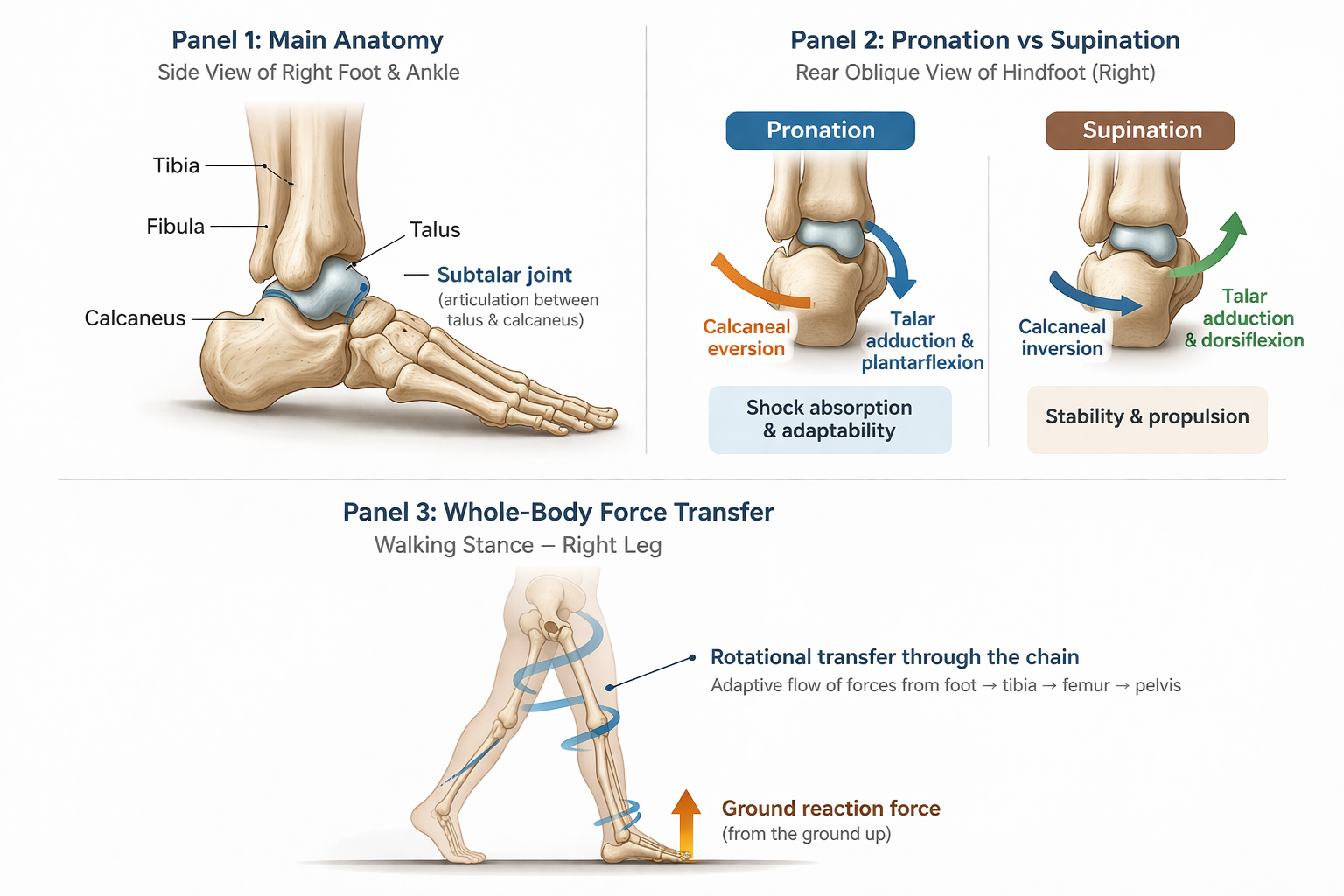
This diagram shows how the talus and subtalar joint help the foot adapt, absorb load and create propulsion, while supporting the transfer of force up through the lower limb during walking.
What the subtalar joint, talus and ground force may be telling your pelvis
When most people think about the pelvic floor, they think about the pelvis.
But often, part of the story starts lower down.
It starts with the foot.
With the way the body meets the ground.
With how it absorbs load, adapts, balances and pushes away again.
Because the foot is not just a base. It is a responsive, moving structure that helps us receive force, organise force and redirect force. The ankle-foot complex is mechanically intricate, and the shape and motion of the talus and surrounding joints play a major role in how movement is transferred through the lower limb.
And right in the middle of that conversation sits the talus and the subtalar joint.
The talus and subtalar joint: small area, big job
The talus is one of the key load-transferring bones between the leg and the foot. It is unusual because it has no direct muscular attachments, so it depends heavily on the shape, motion and support of the structures around it.
Below it, the subtalar joint between the talus and calcaneus helps the foot adapt to the ground. This is not a simple hinge. Its axis is oblique, which means it contributes to the complex combinations of movement we describe as pronation and supination, rather than one neat rolling action.
That matters, because the foot is not designed to stay in one position all the time.
It is designed to change.
Pronation is not bad. Supination is not better.
This is where social media often oversimplifies things.
Pronation is not a flaw.
Supination is not a prize.
In walking, pronation helps the foot become more adaptable and shock-absorbing, while supination helps it become more stable and lever-like for push-off. Gait Happens describes pronation as part of shock absorption and supination as part of stability and propulsion, which is a useful simple summary for a much more complex three-dimensional process.
So the better question is not whether you pronate.
The better question is:
Can your foot move into pronation when you need to absorb force, and then organise into supination when you need to propel?
That is a very different conversation from labelling a foot as flat, collapsed, rigid or bad.
The foot must know when to soften and when to stiffen
A healthy foot is not rigid all the time.
And it is not floppy all the time either.
It needs to yield, adapt and absorb.
Then it needs to organise, stiffen and propel.
That transition is one of the reasons the foot is so important for the rest of the body. When the ankle-foot complex can move well, it helps create more efficient force transfer through the lower limb. When it cannot, something above usually has to compensate.
The difference between sinking into the ground and being supported by it
This is the part I think matters deeply for the pelvic floor.
The goal of gait is not simply to collapse into the floor and hope the body copes.
The body is constantly in relationship with ground reaction force. The ground pushes back, and walking depends on how well we receive and use that returning force. Gait Happens describes efficient foot mechanics as part of smooth weight transfer, shock absorption and propulsion in daily activities.
So the foot is not just there to stop us falling over. It helps determine whether we feel as though we are dropping into the ground or being supported and lifted back out of it.
When the foot can pronate, adapt and spread load, and then reorganise into a more stable, propulsive shape, the body has more chance of receiving support upward through the chain. That is often the difference between feeling heavy and collapsed versus springy and organised. This is partly an inference from known gait mechanics and force transfer principles rather than a direct pelvic-floor study, but it is a clinically useful one.
And when that support is not coming through well, the pelvic floor may end up trying to create stability from the middle.
Why the rotational chain matters
This is the part that often gets missed.
It is not just about rearfoot motion in isolation.
It is about the twist through the foot, the behaviour of the talus, the movement at the subtalar joint, the rotation through the tibia and fibula, the response of the femur, and then the movement options available to the pelvis.
Research supports a relationship between distal foot mechanics and more proximal alignment. In studies of induced hyperpronation, changes in foot position were associated with increased shank internal rotation, thigh internal rotation and anterior pelvic tilt.
So when we talk about the pelvis, we are not talking about a structure floating above the feet in isolation. We are talking about something that responds to the timing and quality of force transfer through the whole limb.
That is also why I think we need to interpret orthotic studies carefully.
Some studies show that orthoses can clearly change hindfoot mechanics while having only limited direct effect on hip and pelvic kinematics. One classic paper found that the principal effects were seen at the hindfoot complex, with much smaller changes at the knee, hip and pelvis.
To me, that does not mean the foot and pelvis are unrelated.
It may simply mean that changing one local variable under the foot does not automatically restore the full three-dimensional rotational sequence of gait. A wedge can alter a local mechanical behaviour, but that is not the same thing as restoring whole-chain timing, sensory input, adaptability and propulsion.
Function matters more than appearance
A foot can look pronated and function fairly well.
A foot can look neat and “neutral” and still move poorly.
That distinction matters.
The relationship between foot posture and symptoms is not always about how the foot looks statically. Research into foot and pelvic alignment suggests that foot mechanics can influence proximal segments, but the body is variable and the relationship is not one-size-fits-all.
So I am much more interested in questions like:
Can you receive weight?
Can you adapt to the ground?
Can you transfer force?
Can you push away without gripping?
Can support travel upward through you?
So where does the pelvic floor come in?
This is where I want to stay careful and honest.
At the moment, the evidence does not prove that pronation or supination directly causes pelvic floor dysfunction.
But there is good reason to think that foot mechanics can influence the environment in which the pelvic floor has to work.
Pelvic floor muscles are active during walking and jogging, and their activity increases with locomotor demand. In a 2022 study, pelvic floor muscle activity was characterised across the gait cycle in continent adults during walking and jogging, supporting the idea that the pelvic floor is part of dynamic load management rather than something that only switches on during isolated exercises.
So if the lower limb is receiving force poorly, rotating poorly, or failing to transition effectively from absorption to propulsion, the pelvis and trunk may need to compensate. And the pelvic floor may end up joining that compensation.
Not because the foot is “causing” it in a crude one-step way.
But because the pelvic floor lives inside a system trying to create support, balance, pressure control, timing and forward movement.
If the body does not trust the support coming from below, it often tries to create safety from the middle.
That can look like gripping.
Or bracing.
Or heaviness.
Or a loss of recoil.
Grounding is not collapsing
A lot of people are told to “ground” through their feet, but what they actually do is sink.
They drop into the arches.
Grip the toes.
Hang in the hips.
Brace through the belly.
And then wonder why the pelvic floor feels heavy or reactive.
True grounding is not collapse.
It is the ability to meet the floor and receive support back.
That means enough pronation to absorb.
Enough sensory awareness to balance.
Enough rotational freedom through the lower limb to transmit force.
And enough later stiffness to create propulsion.
When that is available, the body often feels less like it is holding itself up from the top down.
And more like it is being lifted from the ground up.
What prominent voices add to this conversation
Diane Lee’s educational work is useful here because it treats the body as an integrated system rather than a set of disconnected parts. Her teaching catalogue specifically includes a lecture called The Foot and Pelvic Floor, focused on foot biomechanics and assessment in relation to the lower extremity and squat mechanics.
The Franklin Method adds another valuable layer by emphasising dynamic anatomy, fascia, imagery and coordination rather than rigid positioning. Franklin Method materials specifically describe the connections between hip, leg and foot fascia, and the organisation also lists dedicated pelvic floor fascia training among its trainer pathways.
Gait Happens has done a good job of making foot mechanics more accessible while still keeping function at the centre. Their materials repeatedly highlight shock absorption, stability, weight transfer and propulsion as key features of healthy foot function.
And Antony Lo, The Physio Detective, is a useful figure to know here because his work pushes against overly simplistic structural models and encourages broader clinical reasoning around movement, pain and function.
The bigger takeaway
The goal is not to stop pronation.
The goal is not to hold an arch all day.
The goal is not to force the body into a rigid ideal.
The goal is to create a system that can:
receive force
absorb force
organise rotation
create propulsion
balance without bracing
and let support travel upward through the body
Because a healthy foot does not just stop you from sinking.
It helps the whole body organise enough to rise.
And when the body can trust the ground, the pelvic floor often has less need to grip for safety.
Gentle invitation
If you are dealing with pelvic floor symptoms, it is not always just about the pelvis.
Sometimes we need to look at breath.
Sometimes scar tissue.
Sometimes rib position.
Sometimes nervous system tension.
And sometimes we need to look down at the feet and ask whether your foundation is helping you absorb force, adapt and feel supported from the ground up.
That is part of the work I do inside my 1:1 sessions and programmes. We look at the body as a whole system, so support does not have to be manufactured by gripping from the middle.
Using an exercise band to bring change to the feet
Try this now: two simple ways to wake up the foot
If you want to start exploring this gently, here are two simple exercises you can try right away. One is open chain, where the foot is off the floor and free to move. The other is closed chain, where the foot is in contact with the ground and learning how to organise under load.
1. Open chain: shake hands with your toes
Sit comfortably and bring one foot onto the opposite thigh, or onto a stool if that feels easier.
Thread your fingers between your toes as if you are shaking hands with your foot. Then pause and let the foot soften around your hand.
From there, gently:
move the forefoot a little side to side
circle the ankle slowly
softly spread and wiggle the toes
add a small point and flex
Keep your jaw soft and your breath easy.
This can help improve sensory awareness, create more space through the forefoot, and encourage the foot to feel less rigid and more adaptable.
2. Closed chain: tripod rock and rise
Stand barefoot and place one foot on the floor.
Find three points of contact:
the base of the big toe
the base of the little toe
the centre of the heel
Gently rock your weight forwards and back, then side to side, and then let yourself settle somewhere in the middle.
From there, without gripping the toes, imagine the arch responding gently and the leg growing tall above the foot. Keep the knee soft. Let the foot meet the floor, and the floor meet you back.
You can then add a tiny bend and straighten of the knee without losing that tripod.
This helps the foot learn how to receive load, organise balance, and create support from the ground up rather than collapsing into it.
These are not about forcing an arch or trying to “fix” the foot. They are about giving the body more options. One helps the foot move more freely. The other helps it organise more clearly under load. And both can begin to change the conversation between the ground, the leg, the pelvis and the pelvic floor.
Further reading
Brockett CL, Chapman GJ. Biomechanics of the ankle. 2016. Provides a broad overview of ankle-foot anatomy and mechanics, including the complexity of motion through the ankle-foot complex.
Williams AMM et al. Characterizing Pelvic Floor Muscle Activity During Walking and Jogging in Continent Adults. 2022. Useful for understanding that the pelvic floor is active during gait and not just during isolated exercises.
Khamis S, Yizhar Z. The Relationship Between Foot and Pelvic Alignment While Standing. 2015. Explores the coupling between induced foot hyperpronation and more proximal segment changes, including pelvic alignment.
Nester CJ et al. Effect of foot orthoses on the kinematics and kinetics of normal walking gait. 2003. Helpful for understanding why a local change at the foot does not always create a dramatic pelvic change.
Diane Lee. The Foot and Pelvic Floor. Educational lecture page.
Franklin Method. Fascia Trainer for the Hip, Leg & Foot and Franklin Method trainer pathway pages mentioning pelvic floor fascia training.
Gait Happens. Foot pronation vs supination and Why foot biomechanics matter. Accessible summaries of shock absorption, propulsion and daily movement relevance.
Antony Lo, The Physio Detective. Useful broader clinical reasoning perspective on moving beyond purely structural models.