How the Bladder Really Works: Urgency, Leaks, Pelvic Floor and the Nervous System
Most people think the bladder is the story.
It is only part of it.
Bladder function is really a conversation between the kidneys, ureters, bladder wall, urethra, pelvic floor, spinal cord, brain, fascia, hormones, habits, stress state and everyday life. It is not simply a matter of whether you are “weak”, whether you have remembered to do your squeezes, or whether you are getting older., that would make it so much easier! But no the urinary system depends on storage, sensation, timing, coordination and release.
That matters, because when someone tells me they leak on the way to the toilet, feel constant urgency, dribble after wiping, cannot fully empty, or only seem better when they are on holiday, I do not hear “bad bladder”. I hear a body trying to manage pressure, sensation, timing and safety.
The kidneys start the story
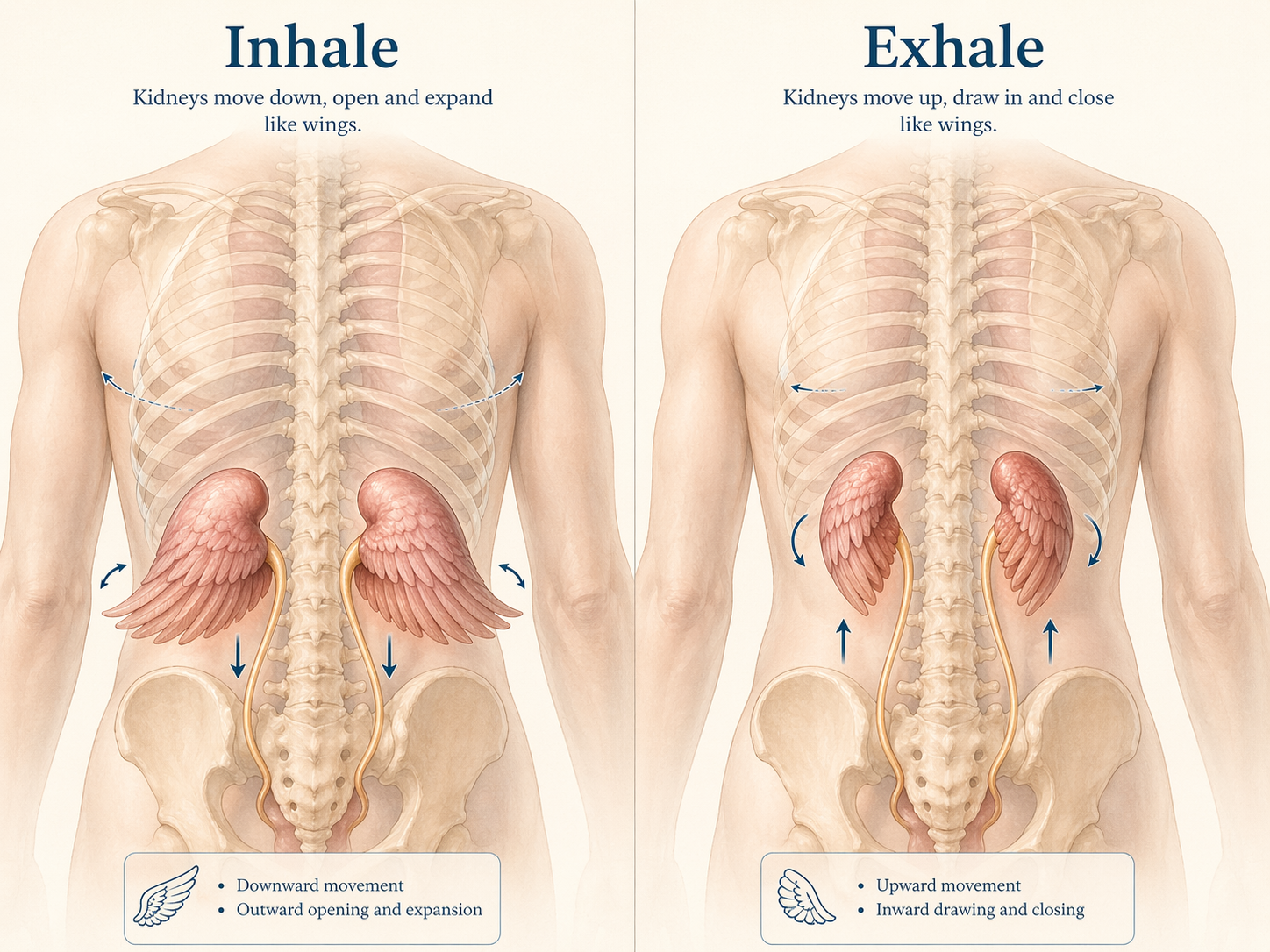
A visualisation of kidney movement with breath: opening and widening on the inhale, gently drawing up and in on the exhale.
Your kidneys are quietly working all day. They filter the blood, balance fluids, salts and minerals, remove waste and make urine. That urine then travels down the ureters into the bladder, where it is stored until the nervous system judges that it is the right time and place to empty. Healthy kidneys filter about half a cup of blood every minute and produce around 1 to 2 quarts of urine each day.
So even though this is a blog about the bladder, it helps to remember that the bladder is receiving what the kidneys have already prepared. Hydration, caffeine, alcohol, salt balance, medications, hormones and general health all influence what reaches the bladder in the first place.
The bladder is not just a bag
The bladder is not a floppy storage sack sitting there waiting to be emptied. Its wall contains the detrusor muscle, and as the bladder fills, stretch-sensitive nerves in the bladder wall and lining send information to the spinal cord and brain about fullness. The best-established “I’m filling” signal comes from the bladder itself, especially through afferent nerve fibres (these send messages to the central nervous system) that respond to distension.
During storage, the detrusor should stay relatively relaxed while the outlet stays closed. During voiding, the detrusor contracts and the outlet, including the urethral sphincter system and pelvic floor, has to let go enough for urine to pass. Good bladder function is not about one muscle being strong all the time. It is about the system being able to switch.
That is one reason the old advice (still often given) to “just squeeze more” so often misses the mark.
The urethra is part of the continence story
The urethra is not just a pipe. It is part of the closure system.
The internal urethral sphincter is made of smooth muscle. It consists of spindle-shaped cells that contract slowly and efficiently and is continuous with the detrusor. The external urethral sphincter is made of striated muscle and is under voluntary control through pudendal nerve pathways. In women, the urethra also sits within a wider support system involving fascia, vaginal tissues, the pelvic floor and the muscles around it. In men, continence is influenced by the urethra, bladder neck, prostate-related structures and the external sphincter system.
So the story is never just “what is the bladder doing?” It is also “what is the outlet doing?” and “can the body coordinate storage and release at the right time?”
When anatomy is not textbook
Most of us are taught a very simple picture of the urinary tract. One kidney draining through one ureter into the bladder on each side, and then one urethra carrying urine out.
But bodies are not always that neat.
Some people are born with a duplicated ureter or duplex collecting system, where one kidney has two drainage channels instead of the usual one. Sometimes those two ureters join before they reach the bladder, and sometimes they remain separate. Many people never know they have it, but in some cases it can be linked with recurrent infections, reflux, unusual leaking patterns, poor drainage, or an ectopic ureter opening in the wrong place.
I think this matters to mention not because everyone with bladder symptoms has a duplicated ureter, but because it reminds us that not everybody’s urinary anatomy follows the neat textbook drawing. Sometimes symptoms are not just about habit, tone or stress. Sometimes the plumbing itself is a little different.
“There are also rarer congenital differences, including accessory or duplicated urethral structures, which are far less common but are another reminder that bodies do not always follow the standard diagram.”
The nervous system is involved in every wee
We do not wee simply because the bladder is full.
We wee when the bladder, spinal cord and brain agree that now is the right time and place to let go. This whole process is coordinated through a network that includes the sacral spinal cord, the periaqueductal grey, the pontine centres and higher brain regions.
The periaqueductal grey, or PAG, sits in the midbrain and helps the brain keep track of internal body signals, including how full the bladder is. The pontine centres in the brainstem then help organise the switch between holding on and letting go, making sure the bladder muscle and the outlet are doing opposite jobs at the right time.
As the bladder fills, reflexes known as the guarding reflex help keep us continent by increasing activity around the outlet.
This is where Onuf’s nucleus becomes especially interesting. It is a specialised group of motor neurons in the sacral spinal cord that helps control the striated muscles of the external urethral and anal sphincters, as well as pelvic floor-related structures. In other words, it sits right in the middle of the body’s “hold on” story.
So continence is not just muscular. It is neurological, reflexive and shaped by lived context.
Does the pelvic floor affect the bladder’s message?
The strongest evidence I can find says that the primary fullness signal comes from stretch-sensitive nerves in the bladder itself. That is the best-established mechanism. But the pelvic floor and outlet system are not passive bystanders. As the bladder fills, urethral pressure normally rises and storage reflexes recruit the outlet system to help maintain continence. There is a bladder-to-urethra and bladder-to-pelvic-floor relationship, not just a one-way message from bladder to brain.
Pelvic floor overactivity, high tone and myofascial tenderness are associated in some patients with urgency, frequency and a sense that the bladder is loud and demanding. A recent paper on myofascial urinary frequency syndrome found pelvic floor hypertonicity and tenderness in the vast majority of that group. In other words, when the pelvic floor is guarded, tender and overactive, the whole urinary picture can become earlier, louder and more urgent.
On the other side, reduced support, prolapse, altered coordination or nerve issues can sit more with leakage, poor emptying, a weak stream, positional voiding, overflow or a less clear sense of fullness. That does not prove a neat “late message because low tone” rule, but it does support the broader idea that the quality of the pelvic floor tissues and their organisation shape how bladder filling is experienced.
So the most honest way I would say this for you all is:
As the bladder fills, the main fullness signal comes from the bladder wall itself. At the same time, the outlet and pelvic floor respond as part of the storage system. The tone, tenderness, support and coordination of those tissues may influence how that filling is perceived. A guarded pelvic floor may sit in the picture of urgency and frequency. A poorly supportive or altered system may sit more with leakage, prolapse, poor emptying or altered awareness. It is not quite as simple as tight means early and weak means late, but clinically that pattern is often not far away from what many of us see and experience.
The amygdala, stress and the holiday effect
The bladder is one of those systems that can get very loud when the body feels under threat.
There is good evidence linking anxiety and stress with worse overactive bladder symptoms and worse bother from urgency and incontinence. People with overactive bladder and anxiety often report more severe symptoms and poorer quality of life. I know this was a real issue for me and is now the only time I feel incontinence issues when I am really stressed or anxious I feel the need to pee much more acutely. When I catch myself and use self talk to quiet the noise the symptoms often fall silent (if I catch myself in time!).
That does not mean symptoms are “all in your head”. It means the brain, body and bladder are in conversation.
This is why I think so many women notice improvement on holiday. Less rushing. Less anticipatory bracing. Less work stress. More sleep. More walking. More time to empty properly. More laughing. More exhaling. I have not found a neat study using the exact phrase “holiday effect”, so I would not dress it up as proven fact. But it fits perfectly with what we do know about stress, attention and lower urinary tract symptoms. And is true of so many of my clients over the years.
Prolapse, scar tissue and why symptoms can feel so mixed
Pelvic organ prolapse is not simply “something dropping” as it is so often described. Prolapse can alter support around the bladder neck and urethra, change the angle of the outlet, affect emptying and contribute to urgency, frequency, weak stream, straining, positional voiding, leakage or retention. Lower urinary tract symptoms are common alongside prolapse, especially when the anterior and apical compartments are involved.
Scar tissue can complicate things as well. Whether after birth, pelvic surgery, abdominal surgery or prostate surgery, changes in tissue glide, sensitivity and local mechanics may affect how the outlet moves and how the nervous system interprets the area. The exact picture varies person to person, but it makes sense that tethered, irritated or defended tissues can change both movement and signalling.
The many ways bladder symptoms can show up
This is where naming helps, not because labels solve anything, but because different patterns often need different support.
Stress urinary incontinence is the leak that comes with coughing, sneezing, laughing, lifting, running, jumping or impact. It tends to reflect a pressure-management and outlet-support problem more than a bladder contraction problem. When people recognise this pattern, it often helps to think less about clenching hard and more about timing, breath, rib movement and how the body handles rising pressure. NICE recommends at least 3 months of supervised pelvic floor muscle training as first-line treatment for stress or mixed urinary incontinence in women. So not just learning off the internet, this is hard though when waiting lists can be months and embarrassment keeping many from seeking help in the first place.
Urgency urinary incontinence is the “I have to go now” leak. It usually arrives with a compelling urge that is difficult to defer. If someone recognises this pattern, bladder training is often part of the answer, alongside reducing unnecessary rushing, noticing triggers, and learning how to let the first spike of urge settle before reacting to it. NICE recommends bladder training for at least 6 weeks as first-line treatment for urgency symptoms. I have included my guide throughout this blog.
Overactive bladder is the larger umbrella under which urgency sits, often with frequency and getting up at night, with or without leakage. In real life it often feels like always thinking about the toilet, always scanning ahead, never quite relaxing. If someone recognises themselves there, it can help to track patterns gently, look at caffeine and constipation, and notice whether they are emptying because the bladder asked or because their mind panicked first. This can be massively helped in my experience with self talk, TRE™️ to help the nervous system recalibrate and Hypopressives to help the body learn how to effectively manage pressure.
Underactive bladder looks very different. The stream may be slow. Starting may be hard. There may be hesitancy, straining and the sense that the bladder never quite empties. When people see themselves in that description, the answer is usually not to push harder. It is often to create better conditions for release. Sitting fully, supporting the feet, softening the jaw and belly, breathing and sometimes using double voiding can help, but persistent symptoms deserve proper assessment. Pelvic floor physical therapy can help some people with retention symptoms by stretching tight muscles and helping them stay relaxed. But if we don’t address what is going on with the nervous system. This is something that we address with TRE™️ and Hypopressives.
Urinary retention is one of the patterns that I would be more cautious with. Acute retention can be painful and urgent. Chronic retention can be quieter and show up as poor emptying, recurrent infections, overflow leakage or frequent small voids. If someone reads that and thinks, “that might be me,” I would not encourage them to simply experiment alone for weeks. Difficulty emptying needs proper assessment, especially if there is pain, a painfully swollen lower abdomen, or an inability to wee at all. Make an appointment. If you want to take a friend with you. But also look at what is occurring in your life. Your levels of stress, autonomy, the private thoughts you don'‘t share with others and ask for help if you need it, or take time out even a couple of hours to be with yourself and ask yourself how you are feeling. Don’t force it just listen and then write down whatever comes up. Then if there actions to take. Take them.
Overflow incontinence is different again. Here the bladder does not empty properly, it becomes too full and then leaks. That is not the same as a cough leak or a sudden urgency leak. If someone recognises that picture, the main thing is not to assume it is a weakness problem. It is to find out why the bladder is not emptying well enough. When the bladder does not empty fully, it is not always a “weak pelvic floor” problem. Sometimes the issue is obstruction, narrowing, prolapse position, nerve signalling, medication, pelvic floor overactivity, or the bladder muscle not contracting well.
This matters because the treatment depends on the cause.
The work I teach, Hypopressives, breath work, pelvic floor release, Franklin Method™️, TRE™️ and whole-body movement can help when incomplete emptying is linked to tension, breath-holding, poor pressure management, nervous system guarding or pelvic floor muscles that cannot relax well.
But it does not replace medical assessment. If there is recurrent infection, pain, straining, a weak stream, or a feeling that urine is left behind, that needs checking by a GP, pelvic health physio, urogynaecologist or urologist.
We are not just trying to “strengthen the pelvic floor.” We are helping the whole system learn when to hold, when to support, and when to let go.
Post-micturition dribble is the little leak that comes after you thought you had finished, usually after you stand up. This is defined as involuntary loss of urine immediately after passing urine, often after rising from the toilet in women. This is one of those symptoms that many people feel embarrassed by even though it is so common. If someone recognises it, slowing down at the end, waiting a touch longer and gently repositioning before standing can help.
Terminal dribble is different. That is the slow final trickle while the void is still happening. It can sit in the same family as hesitancy, straining or weak stream. If that is familiar, I would be more interested in the whole emptying pattern than in telling someone to do more squeezing.
Then there is the “just in case” wee. Not a diagnosis, but a habit that can quietly retrain the system in the wrong direction. When you keep emptying before there is a real urge, the bladder-brain system can begin to signal earlier and earlier. If someone sees themselves in that habit, I would not suggest being rigid or punishing. I would suggest curiosity. Which of those wees are genuinely needed, and which are fear talking? Bladder training guidance is built around reducing that hair-trigger relationship gradually.
And then there is the leak you did not notice. Sometimes it is a tiny stress leak. Sometimes post-micturition dribble. Sometimes overflow. Sometimes the sensory picture is simply muddy. That is where a bladder diary can be so useful, not because it is glamorous, but because it often reveals a pattern the body has been trying to show you all along.
The wee that appears when you stand up after wiping
This deserves its own mention because so many women quietly think they are the only one.
Often this is post-micturition dribble, or a bit of urine left in the urethra or around the outlet that escapes when position changes. Sometimes prolapse, tissue folding, outlet tension, poor emptying or simple rushing are part of it. This is one reason I so often suggest that my clients don’t spring up the second the stream stops. Give it a second or two. Let the body finish. Breathe. Then stand.
Vulvodynia, pain and why “more squeeze” can backfire
Vulvodynia is vulval pain lasting at least 3 months without a specific identifiable cause. NHS guidance describes burning, soreness and stinging, and some NHS pelvic pain resources note that urinary urgency, frequency, pain on urination and incontinence can also overlap with it.
That overlap matters because pain changes tone, tone changes voiding, voiding changes habit, and habit changes signalling. A sore system often becomes a guarded system. And a guarded system does not usually need more force thrown at it.
If someone recognises that mix of vulval pain, urinary symptoms and pelvic floor guarding, I would think softness before strength. Down-training, pain-sensitive pelvic health physiotherapy, reducing irritants, reviewing soaps and friction, and letting the area feel safer again are often more useful first conversations than harder pelvic floor work.
Men are in this story too
Bladder conversations are often written as if only women matter.
Men also deal with urgency, frequency, weak stream, post-micturition dribble, retention, pelvic pain and incontinence. Prostate enlargement can obstruct flow. Prostate surgery can affect sphincter function and lead to stress urinary incontinence. Reviews of post-prostatectomy incontinence make clear how significant this can be.
And yes, pudendal nerve irritation and Alcock’s canal entrapment are worth mentioning. They are not the most common cause of urinary symptoms, but they can be associated with pain, urgency, frequency and voiding dysfunction.
There are holistic ways to give yourself the best start to healing.
There is hope here. These symptoms are not always quick to untangle, but they are definitely not beyond support.
Bladder training can be a really helpful starting point, especially if urgency or overactive bladder is part of your picture, and I have a free document to help with that. But I also think it matters to say this clearly: no one settles a bladder by staying in a body that feels frightened, rushed and braced all day. If your pelvic floor already feels tight, sore, guarded or overworked, then more squeezing may not be the answer yet. Sometimes the first job is to help the system feel safer, softer and more coordinated. That is where Hypopressives, TRE™️ and Franklin Method™️ can come in so perfectly. They can help you to understand and experience how to breathe better, move better, sense more clearly, organise pressure more efficiently, and come out of the sort of gripping that keeps the whole system on high alert. Pelvic floor muscle training still has an important place, especially for stress incontinence, but it works best in a body that can both respond and release. Sometimes we have to create that first.
Franklin Method and the kidneys
I went looking for a kidney exercise because I know how much easier it is for many people to understand the body when they can feel a place rather than just learn a name for it.
Franklin Method™️ has a lovely way of doing that through touch, imagery and movement. One Franklin resource describes the kidneys as gliding slightly down on the inhale and up on the exhale, with gentle movement of the spine helping a person sense the back body more clearly. Franklin presents this as an imagery and movement tool, not as a direct treatment for bladder dysfunction, and I think that is the honest and useful way to hold it.
I would never say kidney imagery cures urgency. But I do think it can soften a rigid upper lumbar area, invite breath into the back ribs and bring someone out of that fixed, held way of standing that so often comes with pelvic floor issues.
Qigong, kidney breathing and the kidney sound
I also found qigong material around kidney breathing and the Six Healing Sounds. In traditional qigong teaching, the kidney sound is often written as “Chui”, with a soft rounded exhale that can sound a little like “whooo”. The exact spelling and pronunciation vary between schools, which is often the way with these ancient traditions.
I want to be careful here too. I am not over promising!! I honestly did not find strong evidence that making a kidney sound directly fixes bladder symptoms or medically “treats the kidneys”. But you never do know…What I did find is broader evidence that practices in the tai chi and qigong family can support mood, stress regulation and autonomic function. That is not nothing. It fits with the wider idea that slowing down, lengthening the exhale and bringing awareness to the back body may help the whole system feel less defended.
So I am not making a grand claim about the magic of ‘whoo’ (did you see what I did there? ).Putting it simply - sound, breath and attention can create better conditions for your whole body system to work.
A combined Franklin and qigong kidney exercise
Try this with an open mind 😊
First take a moment to notice your breath - then do a tiny side bend or a slow turn through the trunk and notice how your breathing feels. Don’t rush this bit, taking a full minute is a great guide.
Stand or sit comfortably. Place one hand around the side of your lower ribs and the other around the back body where your kidneys sit, just below the lower ribs and above the waist. Breathe in gently through the nose and imagine the back of the ribs widening, the waist softening and the kidneys drifting down and broadening with the inhale. Then breathe out with a soft, unforced “chui” or rounded “whooo”, as though you are gently fogging a mirror with softer lips. As you exhale, imagine the kidneys floating slightly upward again and the waist gathering in without gripping.
After doing this a few times you could return to the tiny side bend or a slow turn through the trunk and notice whether the breath reaches the back body a little more easily.
This is not a magic kidney cure. It is simply a way of bringing movement, softness and awareness into an area many of us barely feel at all. Franklin gives us the imagery and anatomy. Qigong gives us slowness, breath and sound. Together, they can help the body feel less braced and more available.
My take
In my own work, I rarely see a bladder problem in isolation.
I see women and men whose bodies have become a little too ready to brace, a little too used to rushing, a little too disconnected from the softer signals of fullness, support and release.
I also see symptoms improve when people feel safer. On holiday. After sleep. After slowing down. After finally understanding what kind of symptom they are actually dealing with. After realising that a leak is not always weakness, and urgency is not always a naughty bladder, and poor emptying is not something to just push through.
The body is always responding to context.
That is not the same as saying symptoms are imagined.
It is saying our environment can affect them, our life situation, and so much more.
A gentle place to begin
If you are not sure where to start, begin here. Sit fully when you wee. Do not hover if you can avoid it. Let your jaw soften. Let the ribs widen as you inhale. As you exhale, do not push. Give the body a second longer than you usually would. Notice whether you are emptying because your bladder asked, or because your mind got there first.
And once or twice a day, place your hands around the lower ribs and upper waist and try the kidney breath with the soft sound. Not because it is a trick. Just because it might help you feel your back body again, and sometimes that is where better coordination begins.
Because the bladder is never just the bladder.
Medical disclaimer - important!
The information in this blog is for educational purposes only and is not a substitute for personalised medical advice, diagnosis or treatment. Please seek medical advice if you have blood in the urine, recurrent infections, significant pain, difficulty passing urine, suspected retention, prolapse symptoms, new unexplained leakage, or persistent pelvic pain.