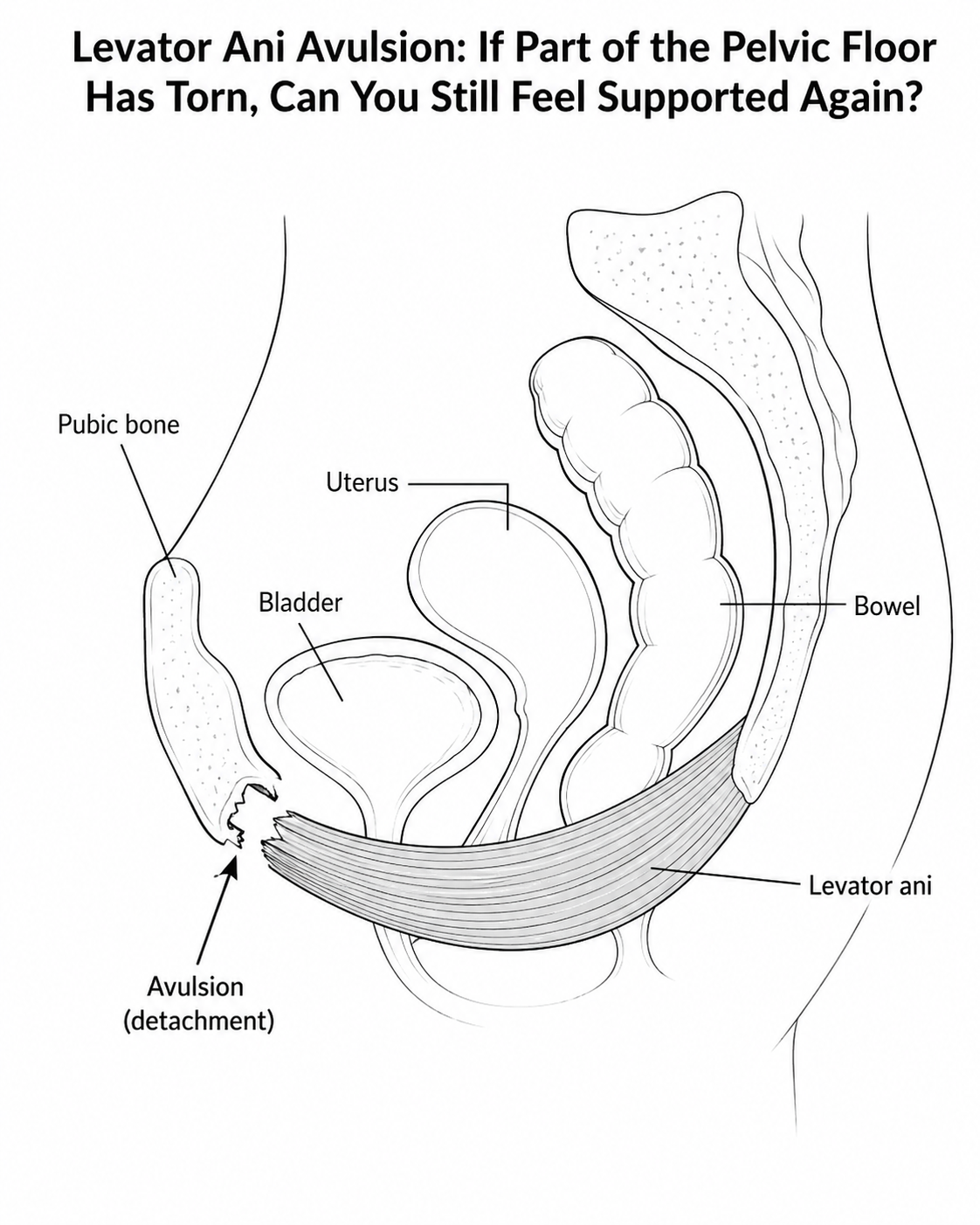
Levator Ani Avulsion: If Part of the Pelvic Floor Has Torn, Can You Still Feel Supported Again?
Being told you have a levator ani avulsion can feel really frightening.
For many women, it lands like a full stop, and feels very, very final.
Something has torn. Something has detached. Something has changed inside my body.
And often the next thoughts are:
Does this mean I am stuck like this?
Does this mean I can’t have sex? An orgasm? Another baby? An active life?
The hopeful answer is that your life and the things you want to do are all still really possible..
A levator ani avulsion is a structural injury, and I never want to minimise that. If part of the levator ani muscle has detached from its bony attachment, exercise cannot magically stitch it back onto the bone. That would be a really dishonest thing for me to say to you.
But what I can say is that your pelvic floor is not one isolated muscle.
Your support system is much more intelligent, layered and adaptable than that.
And while we may not be able to change the fact that an avulsion has happened, we can often change how the rest of the body supports, responds, loads and protects the area around it.
That is where breath, posture, pressure management, Hypopressives, dynamic movement and progressive strength work, and trauma release, can become incredibly useful.
What is the levator ani?
The levator ani is a group of muscles that are part of the deeper pelvic floor. You can think of them as a strong muscular sling or bowl that helps support the bladder, uterus and bowel.
The levator ani attaches around the inside of the pelvis, including near the pubic bone, and it plays a key role in pelvic organ support, continence, sexual function and pressure management.
During childbirth, especially with forceps delivery, a prolonged second stage, or significant stretching of the tissues, part of this muscle can sometimes detach from its attachment point. This is called a levator ani avulsion.
Research links levator ani avulsion with a higher risk of pelvic organ prolapse and pelvic floor symptoms, although symptoms vary hugely from woman to woman. Some women may have an avulsion and few symptoms; others may feel heaviness, dragging, bulging, leaking, reduced vaginal support or a sense that the pelvic floor has lost its “spring.” (PMC)
And this is important:
A diagnosis gives us information.It does not tell us the whole story of your future. Your symptoms and the way you perceive them and feel about them are just as important.
The two-layer support system
One way I like to explain this is by thinking of the pelvic floor as a two-layer support system.
The deeper layer is the levator ani. This is the thicker, deeper muscular hammock that helps hold the pelvic organs.
The lower layer is the perineal support system. This includes the perineal membrane, the perineal body, and the more superficial muscles around the vaginal and anal openings.
The perineal body is especially important. It is the fibrous anchor point between the vagina and anus, and many pelvic floor muscles and fascial tissues connect into it.
So if the deeper hammock has lost some of its support, the lower layer may start to take more load.
This is where some women describe symptoms like:
“I feel heavy lower down.”“It feels like everything is sitting in my perineum.”“I feel like I have to hold myself up.”“I feel more bulgy by the end of the day.”“I feel worse after lifting, walking too long or being constipated.”
That does not mean the body is failing.
It means the body is asking for better load sharing.
Why “just squeeze harder” is not always the answer
This is where the conversation needs to become more nuanced.
If someone has been told they have a pelvic floor issue, they are often told to do pelvic floor squeezes.
Now, pelvic floor muscle training can absolutely help many women with prolapse symptoms, and there is evidence supporting pelvic floor muscle training for pelvic organ prolapse in the general population. (PMC)
But levator avulsion is different.
If part of the muscle has detached from the bone, we cannot simply assume that squeezing harder will restore the missing attachment. In fact, some women with avulsion may already be gripping, guarding or overworking other pelvic floor fibres in an attempt to feel supported.
So the question becomes less:
“Can you squeeze?”
And more:
“Can your whole system support you?”
Can your rib cage move?Can your breath expand?Can your abdominal wall respond without bracing?Can your pelvis find recoil?Can your glutes, hips and deep core share the load?Can you lift without bearing down?Can you cough without everything dropping?Can you move without fear?
Because pelvic floor support is not just about strength.
It is about timing, pressure, coordination and adaptability.
Why pressure management matters so much
Every time you cough, sneeze, laugh, lift, jump, run, brace, strain on the toilet, or hold your breath during effort, pressure moves through your abdominal and pelvic cavity.
Pressure itself is not bad. We need pressure. We are pressure systems.
The problem is when pressure has only one direction: and that’s down.
If the rib cage is stiff, the breath is held, the abdomen grips, the diaphragm cannot move well, the pelvis is tucked under, or the body braces before movement, then pressure may be driven into the pelvic floor and perineum again and again.
For someone with a levator avulsion, that lower support system may already be doing extra work. So repeated downward pressure can leave the perineum feeling more stretched, heavy, tired or vulnerable.
This is why I often start with pressure before I start with strength.
Not because strength does not matter.
It does.
But if we add strength on top of poor pressure habits, we may just create a stronger body that still pushes down.
Where Hypopressives fit in
Hypopressives can be incredibly helpful here, but they need to be described honestly.
They do not reattach a torn muscle.
They do not “fix” an avulsion.
They are not magic.
But they can be a beautiful way to teach the body to reorganise pressure.
In a well-taught Hypopressive, we are looking for:
rib cage expansion
postural length
abdominal wall response
fascial tensioning
pelvic floor reflex
decompression
a feeling of balance rather than bearing down
The apnoea, or breath-hold after the exhale, combined with rib expansion, can create a sense of reducing pressure because it is more evenly dissipated rather than simply pressed down towards the perineum which can be felt like a lift for some and space through the abdominal and pelvic cavity.
But the key is that it should not feel forced. So many times the Hypopressives I see displayed on social media are unrecognisable as the method that I have studied and taught for so many years.And that makes me sad, because so many women (and men) are trying the ‘social media’ version and understandably not getting anything from it or just think it is some weird abdominal fad.
It should not be a harsh abdominal vacuum.It should not be a hard throat closure.It should not be a “suck everything in and hope for the best” exercise.
When taught well, Hypopressives are not about pulling the tummy in. They are not about creating more tension, you should not feel like you are forcing anything.
They are about teaching the ribs, diaphragm, abdominal wall, fascia and pelvic floor to respond together. They are about harmony, fluid activation, encouragement.
That is very different.
Why this matters after levator avulsion
With levator avulsion, we are not simply trying to strengthen one damaged area.
We are trying to ask the rest of the body to become much more supportive.
That might mean helping the intact pelvic floor fibres to respond better.
It might mean improving abdominal wall tone without bracing. Reminding it instead that it is part of a much bigger team.
It might mean working with the glutes, obturator internus, adductors and deep hip stabilisers.
It might mean creating better rib cage movement so pressure does not keep dropping into the pelvis.
It might mean, it usually always is restoring confidence in movement so the nervous system is not constantly guarding.
This is why I love a whole-body approach.
Because the pelvic floor does not live in isolation at the bottom of the body like a little trapdoor.
It is part of a breathing, moving, sensing, reacting system.
Static work is not enough forever
This is a big one.
It is great to start with stillness.
Lying down.Sitting.Kneeling.Standing.Learning how to breathe.Learning how to expand the ribs.Learning how not to bear down.Learning how to feel lift and support again.
But life is not static.
Life is picking up shopping.Walking the dog.Carrying a child.Climbing stairs.Gardening.Lifting weights.Getting off the floor.Sneezing in Tesco.Laughing with friends.Running for the bus.
So at some point, the work has to move.
This is where dynamic Hypopressives become such a powerful progression..
We start asking:
Can you maintain your pressure strategy while your arms move?
Can you step without losing support?
Can you rotate without gripping?
Can you hinge without bearing down?
Can you load one leg?
Can you move from the floor to standing?
Can your body respond before the pressure drops?
That is the bridge between rehab and actual real life.
Progressive loading: building resilience, not fear
Once the body has a better strategy, we need to load it. Our fascia, muscles, ligaments, tendons and other soft tissues need load to function properly.
This is where I feel many women are left in limbo. They are told what not to do, but they are not shown how to return to life.
Do not lift heavy, you are now too fearful to lift or carry your child/children. Even when you really want to.
Do not run, maybe you will step back from teaching your child to ride a bike and watch someone else do it. Or leave that dream of the park run with friends behind you.
Do not jump, you will make excuses to not jump on the trampoline or over the stream or over the homemade pony jumps in the garden or the waves at the seaside.
Do not strain. Now the fear of constipation rises, making constipation more likely.
Do not make it worse. With no real advice on how not too, just an overwhelming fear of maybe/probably just about everything in your life. There is a blog on this theme here if this resonates with where you are at and would like to know more about how your nervous system effects your pelvic floor.
Of course, we need to respect symptoms. But fear-based avoidance does not build any meaningful or indeed any capacity at all.
The body needs progressive loading.
That might look like::
glute bridges
hip hinges
sit-to-stands
carries
step work
rows
squats
resistance training
suspension work
gentle impact preparation
eventually running or jumping progressions if appropriate
Not all at once.
Not going all hard core..
Not by ignoring symptoms.
But gradually, intelligently and with feedback from the body.
The rule I often use is:
If symptoms are worse later that day or the next morning, the load was too much for now.
That does not mean the exercise is bad.
It means the dose, position, breath strategy or timing needs adjusting.
Gentle starting exercises for levator avulsion support
These are not about forcing the pelvic floor to squeeze harder. They are about helping the whole body share pressure, create better support, and reduce downward strain. I would always recommend finding a Hypopressive trainer to guide you, at least for one session.
1. 360° rib breathing
Lie on your back with your knees bent, or sit comfortably with your feet on the floor.
Place your hands around your lower ribs, fingers to the front and thumbs to the back.
As you inhale, feel the ribs gently widen into your hands, front, sides and back. Let the abdomen soften and expand all the way around, like a corset opening or loosening.. Allow the pelvis to very gently respond, as if the sit bones are widening underneath you.
As you exhale, let the ribs soften back without gripping your tummy or squeezing your pelvic floor. Your abdominals will draw back together - think of that idea of a corset gently drawing in.
This helps teach the breath to move around the whole trunk, instead of pushing pressure straight down.
2. Supported Hypopressive prep
Start by lying, sitting or standing. Respect your spinal curves (if you are unsure about this come and book a session)
Take three calm breaths, allowing the ribs to expand gently on each inhale.
After your third exhale, pause holding the air out and gently open the ribs as if you were inhaling, but without taking air in.
You may feel a subtle shift of pressure through the abdomen and pelvic floor. It should feel spacious, not forced.
Hold only for as long as feels comfortable, then breathe in softly and recover.
This can help the body learn decompression, rib expansion and reflexive support without hard squeezing. If you were like “how?’ just now come see me online or in person and let me guide you through.
3. Wall hinge with breath
Stand facing a wall with your hands resting lightly on it.
Soften your knees and send your pelvis back slightly, keeping your spine long.
Inhale into your ribs. As you exhale, gently press your hands into the wall and feel your body recoil back to standing.
This teaches the body to coordinate breath, hips and pressure during a simple functional movement.
4. Glute bridge for pelvic support
Lie on your back with knees bent and feet hip-width apart.
Take a soft inhale into your ribs.
As you exhale, press gently through your heels and lift your pelvis a little from the floor. Keep your jaw soft and avoid gripping your tummy or having your rib cage higher than your pelvis.
Lower slowly.
This helps the glutes and back body join the support system, so the pelvic floor is not left doing all the work.
5. Gentle loaded carry
Hold a light weight, bag or kettlebell in one hand.
Stand tall, breathe softly, and walk slowly across the room.
Notice whether you grip, hold your breath, tuck your pelvis, or feel pressure dropping down.
The aim is not to go heavy at first. The aim is to teach your body to carry load while staying organised and breathing.
These exercises are not a replacement for individual pelvic health assessment, especially if you have been diagnosed with levator avulsion or prolapse. They are gentle starting points to help you notice how your breath, ribs, hips and pelvic floor work together. To book my Pelvic Floor MOT/1:1 combo.
What about pessaries?
This is also worth including because pessaries can be life-changing for some women.
A pessary is a supportive device fitted inside the vagina, usually by a pelvic health physiotherapist, nurse specialist, GP with training, or gynaecology/urogynaecology service.
It can act like a mechanical support, helping to lift or support the pelvic organs so the tissues are not under constant downward strain.
For some women, this gives them the confidence and comfort to move, exercise and rebuild strength.
It is not “giving up.”
It is not a failure.
It is support.
And sometimes support is exactly what the body needs while it learns to trust movement again. Pessaries are widely used in pelvic floor health as a conservative management option for pelvic organ prolapse, although the specific evidence for levator avulsion management is still actually quite limited. (PubMed)
A more hopeful way to look at levator avulsion
If you have been told you have a levator ani avulsion, I really want you to hear this:
Your body has changed, yes.
But change does not mean that there are no ways I can work with you.
It may mean your support strategy needs to change too.
You may need more help from your breath.More movement from your ribs.More support from your hips.More coordination from your abdominal wall.More awareness of pressure.More progressive loading.More rest between efforts.More support from a pessary or pelvic health physio.More patience with your nervous system.
But there are still options.
You cannot squeeze a torn attachment back into place.
But you can teach the rest of the body to become more responsive, more organised and more supportive. Like a community rallying around.
You can learn how to move without constantly pushing down. Which will help to relieve pressure on the pelvic floor.
You can build strength without fear.
You can stop treating your pelvic floor as a single muscle that has failed you, and start seeing it as part of a whole-body system that can still adapt.
Final message
Levator ani avulsion deserves to be taken seriously.
We as women deserve proper assessment, honest information and good pelvic health support.
But we very much also deserve hope.
Because recovery is not always about restoring the exact structure you had before.
Sometimes recovery is about creating a new support system. One that has lain dormant potentially since your early/pre teens.
One that includes your breath, your ribs, your hips, your abdominal wall, your fascia, your nervous system, your pelvic floor, your strength, and your confidence.
Not one muscle working harder.
A whole body learning to support you again. A re-eduction. Instead of seeing levator ani avulsion as a curtain call, let's change that story and see it as the start of a journey into a better understanding of how your whole body works. Discover how to work with me here.
I am very much looking forward to it.