How Knee Mechanics Affect the Pelvic Floor | Hypopressive Scotland
Why the way your knee bends may influence your hips, pelvis and pelvic floor
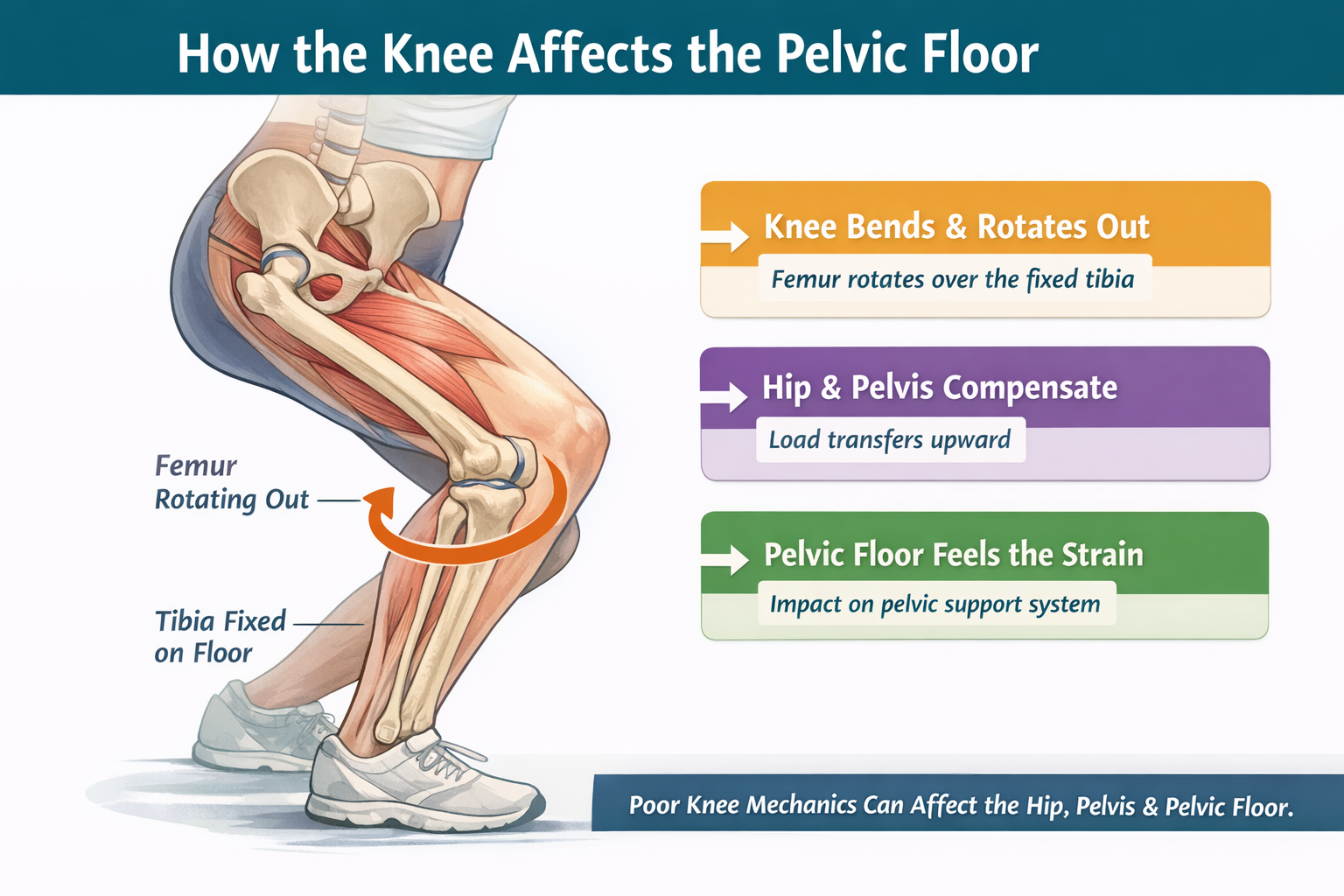
When the foot is grounded and the knee bends, the whole chain above it has to organise well. That includes the hip, pelvis and the support system of the pelvic floor.
Most people think of the knee as a simple hinge.
It bends. It straightens. Job done.
But the knee is far more interesting than that.
Every time you walk, squat, climb stairs, lower into a chair, step off a kerb or lunge forward, your knee is not just bending and straightening. It is also making tiny rotational adjustments that help it lock, unlock and transfer load well. Those small movements matter because the knee does not work in isolation. It sits between the foot and the hip, and what happens there can travel upward into the pelvis and change the environment the pelvic floor has to work within.
This is one of the reasons I am now also very interested in the knee when someone has pelvic floor symptoms. If the leg is not absorbing and transferring force well, the pelvis often has to compensate. And when the pelvis compensates, the pelvic floor often does too.
First, what do open chain and closed chain mean?
These terms sound technical, but they are actually quite simple.
Open chain means the foot is free. It is not fixed to the floor. Think of sitting on a chair and straightening your knee, or lying down and bending and straightening the leg in the air. In this situation, the lower leg can move more independently.
Closed chain means the foot is fixed. It is planted on the floor or against a surface. Think of a squat, a lunge, walking downstairs, or standing up from a chair. In this situation, the body has to organise itself over the grounded foot.
That matters because the rotational story of the knee is described a little differently depending on which part is fixed and which part is moving.
In open chain, we usually describe the tibia moving on the femur.
In closed chain, we usually describe the femur moving on the tibia.
So sometimes two people are describing the same overall relationship, but naming a different bone.
The knee is not just a hinge
The knee has long been taught as a hinge joint, but it is more accurate to think of it as a joint that bends, glides and subtly rotates. One of the classic concepts here is the screw-home mechanism, which helps the knee become more stable near the end of extension and then unlock as flexion begins. This mechanism has been studied in gait and other dynamic tasks, and while real-life movement is more complex than a textbook diagram, that small rotational component is still an important part of healthy knee mechanics.
In the classic teaching model, when the leg is in open chain, knee extension is associated with external rotation of the tibia, and knee flexion is associated with internal rotation of the tibia.
When the foot is fixed in closed chain, the same relationship is described from the thigh bone’s point of view. In that case, knee extension is associated with internal rotation of the femur, and knee flexion is associated with external rotation of the femur.
So if you have heard that the femur spirals out in flexion and spirals in in extension, that fits the classic closed-chain description quite well.
But real movement is never just a textbook
This is where the conversation becomes really useful.
In real life, the femur does not move in a perfect, isolated way. The amount and quality of its rotation will be influenced by the foot, the ankle, the hip, the depth of the bend, the person’s structure, the speed of the movement, and whether they feel safe enough in the task to yield into it rather than brace through it.
As the knee moves from extension into flexion, it has to unlock through a small rotational change. In open chain, this is usually described as the tibia rotating in. In closed chain, it is usually described as the femur rotating out over the fixed tibia. If that subtle rotational glide is poorly controlled, the load can be passed up the chain into the hip, pelvis and the tissues that support the pelvic floor.
Why the knee matters to the hip
When the foot is on the floor and the knee bends, the femur has to rotate and glide well over the tibia. If that movement is stiff, excessive, poorly timed or borrowed from somewhere else, the hip often has to pick up the slack.
That matters because the ligaments and capsule of the hip help manage rotational restraint. They are not just passive wrapping. They guide motion and contribute to stability, especially toward the edges of range. Research has shown that the hip capsular ligaments make a substantial contribution to controlling hip rotation.
So if the knee and femur are not sharing load well, the hip may start to work harder in less efficient ways. Some people collapse inward. Some grip the outer hip. Some tuck the pelvis. Some brace through the ribs and abdomen. Some lose the spring of the foot and ankle and become a little more rigid all the way up the chain.
And this is where the pelvic floor becomes part of the story.
The pelvic floor does not sit outside the chain
The pelvic floor is not an isolated hammock at the bottom of the body. It is part of a whole system of breath, pressure, fascia and movement.
One of the most interesting anatomical links here is the relationship between the obturator internus and the levator ani. These tissues share a broad area of obturator fascia, which means the side wall of the hip and the pelvic floor are not strangers to each other. There is meaningful anatomical continuity there. Recent anatomical work has highlighted this relationship and suggested that dynamic movement of the obturator internus may cooperate with the levator ani through the shared fascia.
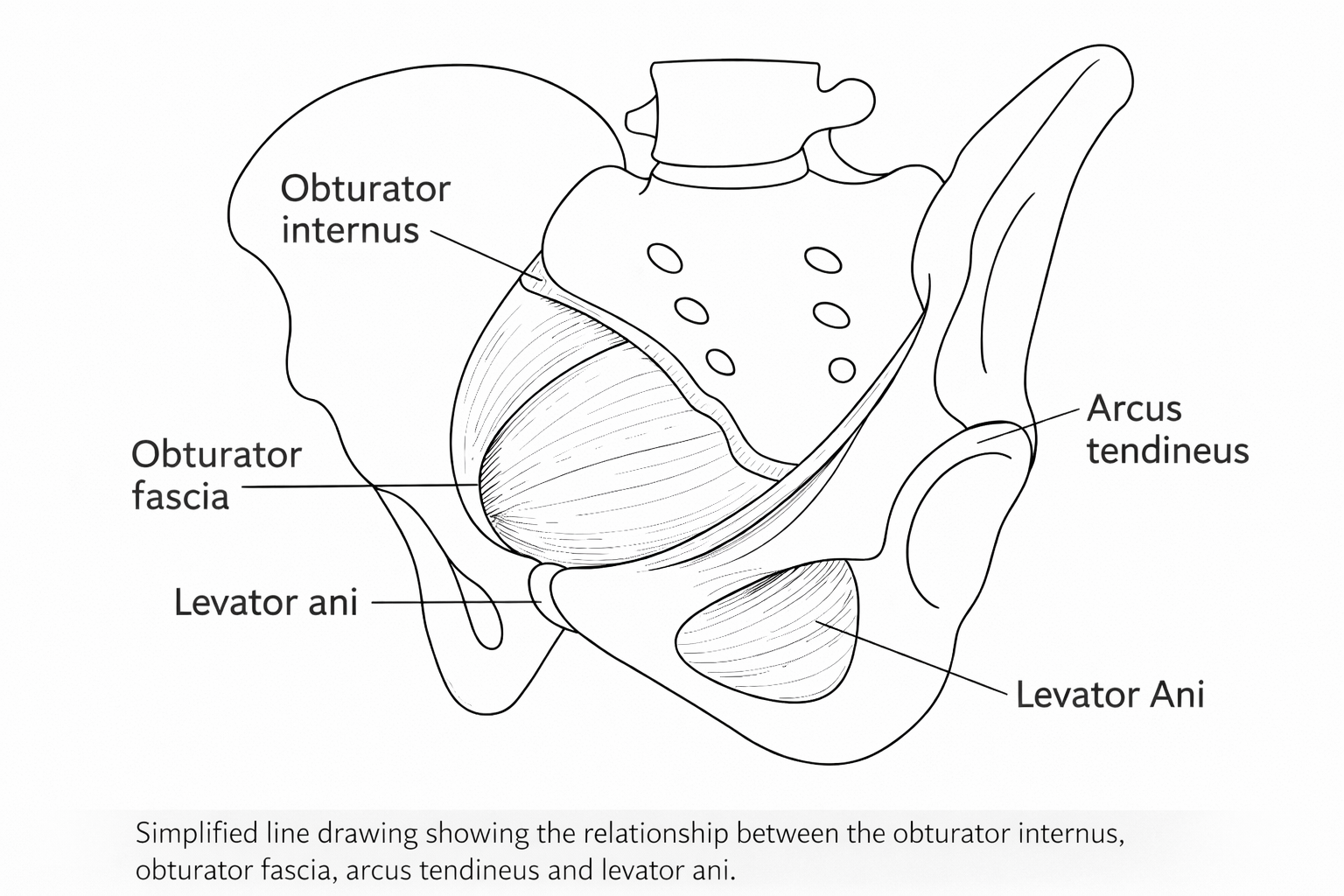
Simplified line drawing showing the relationship between the obturator internus, obturator fascia, arcus tendineus and levator ani.
That does not mean every poorly tracking knee causes pelvic floor dysfunction.
But it does mean that hip mechanics, lateral pelvic wall behaviour and pelvic floor support should not be treated as completely separate conversations.
If the knee is not unlocking and loading well, and the hip is being repeatedly pulled into a poor strategy, then the pelvic floor may end up responding to that wider environment. It may grip. It may lose timing. It may feel heavy. It may become less responsive. It may struggle with impact, urgency, leaking or a sense of dragging. Not because it is lazy, but because it is trying to manage the forces it is living inside.
What I often see in practice
When someone bends through one leg poorly, the issue is rarely just at the knee.
Often the foot is stiff or collapsing.
The ankle does not give enough.
The femur does not rotate well.
The hip hangs into passive tissues or grips for dear life.
The pelvis shifts, tucks or braces.
The ribs stop moving.
The breath becomes shallow or held.
And from there, the pelvic floor has to decide what role it is going to play.
It may overhelp.
It may hold on.
It may fail to recoil well.
It may become reactive rather than responsive.
Interestingly, some research has found that women with urinary symptoms may have weaker hip external rotators and abductors even when pelvic floor strength itself is not significantly different from controls. That is such an important reminder that symptoms are not always about the pelvic floor alone. Sometimes the wider system around it is part of the picture.
Why this matters for the way we train
This is why I do not jump straight to “squeeze more.”
If someone leaks in lunges, feels heaviness on stairs, struggles in squats, or feels unstable on one leg, I want to know more than whether they can contract their pelvic floor.
I want to know:
How is the foot loading?
Can the ankle bend?
Can the knee unlock well?
Can the femur rotate and glide without collapse or gripping?
Can the pelvis stay organised without bracing?
Can the ribs still move?
Can the person breathe?
Because a pelvic floor that is living in a poorly organised system will often behave like a poorly organised pelvic floor.
That is why work on the feet, knees, hips, breath and pressure can be so powerful. Sometimes what helps the pelvic floor most is not a stronger squeeze. Sometimes it is a better conversation between the ground, the leg, the pelvis and the breath.
A simple way to explain it
When your foot is in the air, the shin bone does more of the obvious rotating. When your foot is on the floor, the thigh bone has to rotate over that grounded leg. That tiny twist helps the knee lock and unlock properly. If the twist is missing, excessive or poorly controlled, the hip and pelvis often have to compensate, and the pelvic floor may feel the effect of that.
Final thought
The knee is not just a hinge.
It is an amazing bending, gliding, subtly rotating joint that helps us transfer load through the whole body. When that small rotational story is working well, the hip, pelvis and pelvic floor often have a better foundation to respond from. When it is not, the body may start borrowing from elsewhere.
If you are dealing with leaking, heaviness, gripping, instability or discomfort in movements like squatting, lunging, walking downhill or climbing stairs, it may be worth looking at the knee a little more closely.
Not in isolation! If you have read my blogs before you will know just how crazy it makes me when we look at the pelvic floor or any part of our body as working in isolation. Because we are a global system. So, if we are looking at the knee and pelvic floor, we may also need to look at the hip flexors, the adductors, your feet!
Because a lot of the time the pelvic floor is not the starting point of the problem. Often times it is the place that reveals that there is a problem somewhere in the chain…and that could be your knee.
If you want to explore this connection for yourself, these three simple exercises can help you feel the difference between open-chain and closed-chain knee movement, and notice how the knee, hip, pelvis and breath work together. Or you can take some time to explore your knees with me in this Franklin Method™ - workshop
1. Supported knee glide with foot grounded
This helps someone feel closed chain knee bend more clearly, with the foot fixed on the floor.
Stand facing a wall or kitchen counter and lightly hold on for balance. Place one foot a little in front of the other. Keep the whole front foot on the floor. Slowly bend the front knee forwards over the middle toes, then come back out again.
As you do this, notice:
does the foot stay connected
does the knee track smoothly
does the thigh feel as though it can rotate and soften into the movement rather than collapse
can the pelvis stay quiet without gripping the bottom
Think of the leg accepting your weight rather than dropping into it.
Repeat for 8 to 10 slow reps each side.
Why it helps:
This gives you a chance to explore how the foot, ankle, knee and femur organise together when the foot is fixed. It can also show you whether you brace through the pelvis or hold your breath when load comes into one leg.
2. Seated knee bend and straighten
This is a simple way to explore open chain movement, where the foot is free.
Sit tall on a chair with both feet on the floor. Lift one foot slightly so the lower leg is free. Slowly straighten the knee a little, then bend it again.
Let it be soft and easy. No gripping in the thigh. No forcing.
As you move, imagine the lower leg gently spiralling in as the knee bends and out as it straightens. You do not need to make a big twist. Just sense that the knee is not a dead hinge. It has a subtle rotational story built into it.
Repeat for 8 slow reps on each side.
Why it helps:
This lets you feel the difference between an open-chain leg movement and a closed-chain one. It can be a lovely teaching tool before moving into standing work.
3. Small split-stance bend with breath
This brings the knee, pelvis and breath together.
Stand in a short split stance with one foot forward and one foot back. Keep most of your weight through the front foot. Let the back heel be light if needed. Inhale gently into the sides of the ribs. As you exhale, soften the front knee into a small bend. Then return to standing.
Keep it tiny. Keep the shoulders soft. Let the ribs widen rather than lift. Let the pelvis stay responsive rather than tucked.
As you bend, notice whether:
the foot can stay grounded
the knee can soften without wobbling inward
the thigh can accept rotation without gripping
the breath stays easy
the pelvic floor feels less braced
Repeat for 6 to 8 reps each side.
Why it helps:
This starts to connect pressure, load transfer and knee mechanics. It is often in movements like this that people begin to notice whether the pelvic floor is reacting to the way the body is organising above and below it.
These exercises are not about forcing the knee to move in a certain way. They are about noticing how your body organises load, rotation and breath, and whether your pelvis and pelvic floor respond by softening, bracing or gripping.
Next Steps
If your pelvic floor symptoms show up most when you squat, lunge, walk downhill, climb stairs or spend time on your feet, it may not be just about the pelvic floor itself. The way your feet, knees, hips, pelvis and breath work together matters too.
In my 1:1 sessions, I look at the whole body, not just one symptom in isolation. We explore how you move, how you manage pressure, where you may be gripping, and what your body may need in order to feel more supported from the ground up.
If you would like help understanding your own pattern, you can book a 1:1 with me and we can look at it together.
FAQS
-
They can influence it, yes. The knee sits in the middle of a chain between the foot and the hip. If the knee is not bending and rotating well, the hip and pelvis often have to compensate. That can change how load and pressure are managed, which may affect how the pelvic floor responds.
-
Not necessarily. It is usually more helpful to think of the body as a connected system. Sometimes the pelvic floor is part of the problem. Sometimes it is responding to what is happening elsewhere. The knee may be one piece of the picture rather than the whole answer.
-
Open chain means the foot is free, like when you are sitting and straightening the leg. Closed chain means the foot is fixed, like in standing, squatting or walking. This changes how the bones move and how the body transfers load.
-
No. It behaves like a hinge in some ways, but it also has subtle rotation and glide. That small rotational component helps the knee lock and unlock well, especially in walking and bending tasks.
-
It can. Sometimes that inward movement reflects poor timing or control through the foot, hip or pelvis. Sometimes it is not a problem at all. The key is whether the movement is controlled, comfortable and well shared through the system, or whether it comes with gripping, pain, leaking, heaviness or instability.
-
For some people, yes. If symptoms are linked to how they load one leg, bend, squat, walk or manage pressure, improving the wider mechanics of the foot, knee, hip, ribs and breath can make a real difference.
-
Not always. Sometimes more squeezing is not what the body needs. Sometimes it needs better timing, better breath, better load transfer and less gripping through the surrounding system.