When the Vaginal Opening Feels Wider: Prolapse, the Levator Hiatus and Why It Is About More Than Your Pelvic Floor

a woman standing at a cave entrance - in this blog the cave represents the levator ani hiatus and pelvic health
I still remember the appointment.
After months of feeling heaviness, dragging and all the uncertainty that comes with prolapse, a pelvic health physiotherapist examined me and told me that my opening was wider than she would have expected. She explained that my prolapse itself was helping to hold the opening open and suggested that I consider using a pessary.
Essentially my prolapsed organs were acting like a physical wedge. When the vaginal walls descended, they were physically sitting inside the hiatus, mechanically preventing the levator ani muscles from contracting fully or closing efficiently.
She also asked me to do something that has stayed with me ever since.
“Imagine you are closing your labia like two heavy curtains.”
I tried. And failed. Not because I couldn’t do it. Not because I wasn't trying hard enough, but because, as she pointed out, I couldn't do it without also recruiting my upper abdominal wall and my ribs. I was doing this because when the deep pelvic floor loses its baseline tone, the brain frantically searches for stability elsewhere, usually by over-gripping the upper abs. This actually increases downward pressure on the hiatus- the exact opposite of what you want in this scenario!
At the time, I found that frustrating. Surely my pelvic floor should just work?
Years later, after training in Hypopressives, the Franklin Method, Pilates and TRE®, I see things rather differently. That appointment was one of the first times someone helped me understand that my pelvic floor wasn't simply a flawed part of me. It was simply part of a much bigger system.
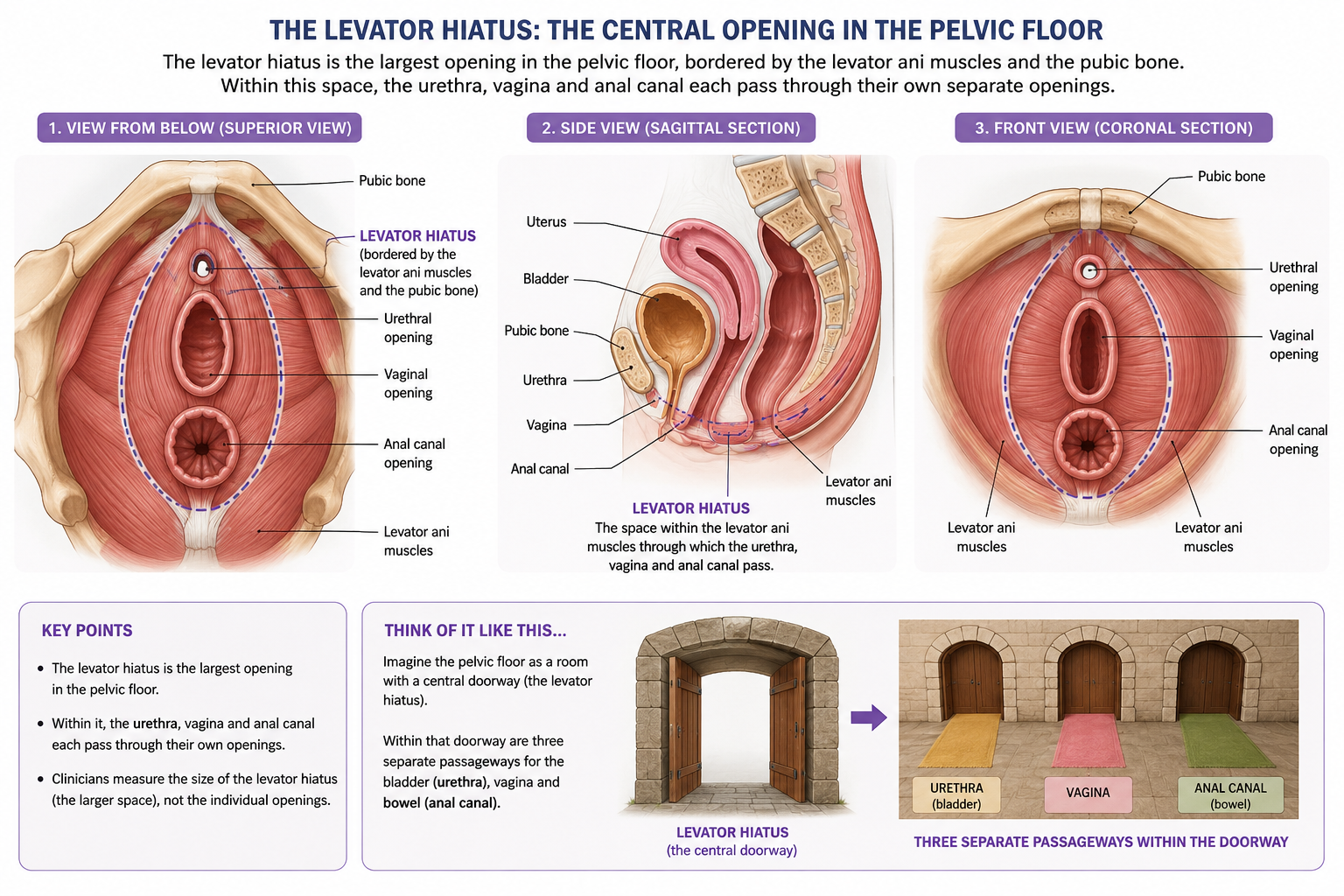
First things first: what is the levator hiatus?
The levator hiatus is the central opening bordered by the levator ani muscles and the pubic bone. Within this wider space, the urethra, vagina and anal canal each pass through their own separate openings and supporting tissues; they do not all travel through one single hole. You can think of the levator hiatus as a shared doorway or central frame, with three distinct passageways arranged within it. When clinicians measure the levator hiatus on imaging, they are measuring the size and shape of that larger muscular opening, not simply the visible vaginal opening itself.
It is not supposed to stay tightly shut.
It widens when we breathe in. It responds when we walk, run, cough and lift. During birth, it expands enormously. A healthy pelvic floor is not rigid; it is adaptable.
When women talk about feeling “more open”, they may be describing several different things:
The visible vaginal opening.
The position of the pelvic organs.
The deeper opening in the pelvic floor muscles.
Changes in muscle tone.
Changes in connective tissue.
A feeling of heaviness or lack of support.
These are not all the same thing, but they are all connected.
Levator ani hiatus as an anatomical image and as a metaphor of single dorrways from a large hall
Why can the opening become wider?
Pregnancy and birth are the obvious reasons.
For nine months, your body changes to accommodate a growing baby. Hormones soften connective tissue. Your breathing mechanics alter. Your centre of gravity shifts. Then, during birth, the pelvic floor has to stretch in extraordinary ways.
For some women, particularly after forceps deliveries, large babies or prolonged pushing, the muscles and connective tissues may remain altered.
Menopause can bring another layer of change. Oestrogen influences collagen, muscle and tissue health, and many women notice symptoms changing during this time. Discover more about how Hypopressives support the nervous system and tissues during menopause
But there are other factors that can increase the size too.
Frequent constipation.
Chronic coughing.
Frequent breath holding under load - not the intentional apnoea of Hypopressives, but the more forceful Valsalva technique often used when lifting, pushing or straining. To learn how to safely manage load without forceful straining, read about finding the middle ground between coordination and pressure.[1]
Years of “holding yourself together”.
Poor sleep.
Stress.
A body that no longer trusts itself.
Because the reality is that prolapse is rarely just about the pelvic floor.
The surprising role of prolapse itself
One of the most interesting things my physio said was that my prolapse was helping to keep the opening wide.
At first, that sounded strange.
But if the vaginal walls or pelvic organs are sitting lower, they may mechanically change how the muscles around them can respond. This is one reason some women find that a pessary immediately changes how their body feels and moves.
A pessary can provide support to the tissues and, for some women, create a better environment for exercise and rehabilitation.
I chose not to use one.
That wasn't because I think pessaries are wrong. Quite the opposite. I have seen them transform women's lives, allowing them to exercise, walk, run and simply feel much more comfortable.
I simply wanted to see what rehabilitation could achieve first.
And what I discovered was that my recovery had very little to do with squeezing harder.
The pelvic floor doesn't work alone
The “heavy curtains” cue taught me something important.
I could make something happen, but I was doing it by gripping through my ribs and upper abdominals, while the lower abdominal wall barely joined in. In other words, I was bypassing the part of the system that should have been coordinating with my pelvic floor.
That was one of the first clues that this was not simply a weak pelvic floor. It was a coordination problem.
Today, we know that the pelvic floor works as part of a team - Deep Core Cylinder or Intra-abdominal Pressure System:
The diaphragm.
The abdominal wall.
The deep back muscles.
The hips and glutes.
The feet.
The nervous system.
The way we breathe and manage pressure.
This is one reason that simply telling women to “do your Kegels” often falls short.
The question isn't always:
“How do I strengthen my pelvic floor?”
Sometimes the better question is:
“What is stopping my pelvic floor from doing its job?”
Does a wider opening affect prolapse?
Research suggests that women with larger hiatus measurements may be at greater risk of prolapse progression and, in some cases, prolapse recurrence after surgery.
But hiatus size is only part of the story.
I have worked with women whose openings appear relatively wide but who have very few symptoms, and others whose prolapses are small on paper but hugely affect their confidence and daily lives.
Symptoms are influenced by:
Physical factors: Tissue quality, muscle strength, coordination, and movement patterns.
Systemic factors: Hormones, breath mechanics, and bowel habits.
Lifestyle factors: Stress levels, sleep, and nervous system regulation.
Human bodies are wonderfully complex, aren’t they?
What if I have a levator avulsion?
This is an important piece of the puzzle that often gets missed.
During some vaginal births, particularly forceps births, prolonged pushing or births involving larger babies, part of the levator ani muscle can partially or completely detach from the pubic bone. This is called a levator avulsion.
Not everyone with prolapse has an avulsion, and not everyone with an avulsion develops bothersome prolapse symptoms. But it may help explain why some women feel that no amount of "doing their exercises" has completely changed the shape of their pelvic floor.
That does not mean recovery is impossible.
Far from it.
Many women with levator avulsion return to running, lifting, sex, sport and active lives. It simply means that rehabilitation may need to focus less on "fixing" anatomy and more on building strength, coordination, tissue tolerance and confidence.
Recent imaging studies, using both MRI and dynamic 3D/4D pelvic floor ultrasound, continue to show that the size and integrity of the levator ani muscles are linked to prolapse recurrence and symptoms after surgery, reminding us that prolapse is about much more than one weak muscle.
What does the research actually say?
The research around prolapse has become much more interesting in recent years because it is moving away from the overly simple idea that stronger always equals better.
We know that women with larger hiatus measurements are at greater risk of developing prolapse and may have a higher chance of recurrence after prolapse surgery. But we also know that pelvic floor muscle training can make a genuine structural difference.
A recent systemic review looking at women with stage I to III prolapse found that targeted pelvic floor training was associated with:
Significant improvements in pelvic floor muscle strength.
Better support and anatomical position of the bladder neck.
Reductions in the physical size of the levator hiatus at rest.
Reductions in how much the hiatus balloons or opens during bearing down.
For more details on how these prolapse stages and muscle behaviors are formally evaluated, you can explore the evidence-based guides provided by the International Urogynecological Association.
The fascinating mismatch
Interestingly, improvements in symptoms do not always match improvements in anatomy.
This matters immensely because many women spend hours peering into mirrors or deeply worrying about what they can see. The reality is that your prolapse symptoms are influenced by far more than just what your anatomy looks like on a medical chart.
Your everyday comfort is dictated by a dynamic combination of your breath, posture, whole-body strength, connective tissue health, and hormones. It is shaped by how your nervous system responds to stress, how confidently you move, and how much daily physical load your body is being asked to tolerate.
All of these things matter.
This is also why I increasingly think that we are asking the wrong question. The question shouldn't be: "How do I close my hiatus?"
Instead, the better question is: "How do I help my body become more adaptable?"
Because life will always involve physical pressure. The answer is rarely to avoid it, shrink from it, or hide from it. The answer is to build a body that knows how to organise it.
Can you improve closure without a pessary?
For many women, yes.
But I think we need to be careful with our language.
The aim is not to permanently close the opening or to hold tension in the pelvic floor all day long.
Healthy pelvic floors need to widen, soften, recoil and support.
What we are really trying to improve is responsiveness.
Can the muscles work with the breath?
Can the hips share load?
Can the body adapt when you pick up your toddler, run for the bus or trampolining with your children?
Can the tissues recover after challenge?
That is a very different goal from simply gripping.
Three simple exercises to begin with
1. Explore your 360-degree breath
Lie comfortably on your back with your knees bent.
As you inhale, allow the ribs to widen into the floor, into your sides and towards your back. Notice whether your neck softens and your jaw unclenches.
As you exhale, allow the breath to leave naturally and notice the gentle recoil through the abdominal wall and pelvic floor.
No forcing.
No squeezing.
Just curiosity.
2. The Franklin Method “heavy curtains” exercise
Lie on your back in a hook lying or semi-supine position with your pelvis resting on two small balls or cushions.
Allow your legs to gently open out to the sides.
Then imagine the tissues around the vaginal opening, the inner thighs and the deep hips helping guide your legs back towards the middle.
Think of drawing two heavy curtains together rather than clenching or gripping.
The movement should feel smooth and coordinated.
3. A small bridge
Lie on your back with your knees bent.
Breathe in.
As you exhale, slowly lift into a gentle bridge.
Notice your hamstrings, glutes and abdominal wall joining the effort.
Lower down with control.
Again, the aim is not to isolate the pelvic floor but to help the whole system share load.
Where do Hypopressives fit?
People often ask whether Hypopressives “lift organs”.
That has never sat comfortably with me.
What I have found, both personally and professionally, is that Hypopressives offer something much broader. They alter pressure dynamics using an abdominal vacuum. Explore the step-by-step synergy of 360-degree lateral breathing and the apnoea phase to understand how this lift works.
They invite us to explore posture, rib mobility, breath mechanics, pressure organisation and movement variability.
At the International Hypopressives Council, we increasingly talk less about reducing pressure and more about helping the body reorganise it.
Because life involves pressure. A lot of pressure sometimes, and pressure is not the enemy! The pressure we create when we lift heavy babies and shopping bags. When we run, laugh and jump isn’t something we need to brace against or fear. This pressure helps us to support our spine, create a functional pelvic floor and stay upright.
The goal isn't to avoid it.
The goal is to help the body respond to it with efficiency, resilience and confidence. And Hypopressives helps us do this in such a beautiful way. We learn to balance and organise posture, becoming aware of how much this influences not just our pelvic floor, but our breath, our mood, our digestion and our mobility.
Hypopressives bring an awareness too to the influence of breath and breathing on our pelvic floor but also our energy levels, our mood, our sleep and the apnoea breath then helps us to re-organise pressure, creates an environment where our lymphatic system gets an extra squeeze.
The apnoea phase creates a unique physiological environment within the body. Emerging research into intermittent hypoxia suggests that carefully dosed fluctuations in oxygen availability may activate pathways involved in mitochondrial adaptation, cellular repair and neuroprotection.
Much of this work comes from fields such as neurology and exercise physiology, where researchers are exploring the effects of intermittent hypoxia on conditions including Parkinson's disease, as well as on human performance and resilience.
Although this research has not been carried out specifically on Hypopressives, it offers a fascinating glimpse into the ways that breath, posture and movement may influence far more than our pelvic floor alone.
For me, this is one of the most exciting aspects of Hypopressives. They are not simply exercises for the pelvis. They invite us to explore the relationship between pressure, posture, breathing, energy, mobility and the remarkable capacity of the human body to adapt.
Then the poses are carefully designed to engage your muscle chains and fascia lines in a progressive way helping to support your breath, your posture and your dynamic functional movement patterns to make life easier, stronger and you much more adaptable.
A final thought
I didn't “fix” my body.
"I didn't magically restore my anatomy to how it looked before children."
What changed was my relationship with my body.
I learnt how to breathe differently. I moved differently. I became stronger. I stopped seeing my pelvic floor as a part of my body that needed annexed off.
Today, I can run, lift, jump, teach and live my life without constantly worrying about my prolapse.
My body is not the same body it was before children.
But it is a body that has adapted.
And perhaps that, rather than perfect anatomy, is what recovery really looks like.
if you would like to work with me start with a pelvic floor MOT -
A comprehensive assessment designed to uncover what may be contributing to your pelvic floor symptoms and create a clear, personalised starting point for recovery.
Your MOT includes:
A detailed pelvic health, lifestyle and movement questionnaire
A video submission so I can assess your breathing, posture and movement patterns
Detailed personalised feedback with starter exercise ideas
A 1:1 session to talk through my findings and put your recovery strategy in place
Together, we’ll explore how your breath, posture, movement, nervous system and whole-body load sharing may be influencing your symptoms. The aim is not to reduce pressure or “lift” pelvic organs, but to help your body generate, distribute and respond to pressure more effectively.
You’ll leave with a clearer understanding of your body and practical next steps tailored to you.
Further reading and research
The ideas explored in this article are drawn from a combination of current research, clinical guidelines, professional training and personal experience. If you would like to delve deeper, these papers and resources provide a good starting point.
Pelvic floor muscle training and prolapse
Systematic reviews suggest that pelvic floor muscle training can improve symptoms of pelvic organ prolapse and may influence the size and function of the levator hiatus in some women.
NICE. Urinary incontinence and pelvic organ prolapse in women: management (NG123), 2019.
NICE. Pelvic floor dysfunction: prevention and non-surgical management (NG210), 2021, updated 2025.
Recent systematic review: The effect of pelvic floor muscle training on levator hiatus morphology and pelvic floor function in women with pelvic organ prolapse (2025).
Pessaries and conservative management
Current guidance suggests that vaginal pessaries can be offered to women with symptomatic prolapse either alone or alongside pelvic floor rehabilitation.
NICE guideline NG123: recommendations on pessaries and pelvic floor muscle training.
NICE guideline NG210: conservative management of pelvic floor dysfunction.
Hypopressives and intra-abdominal pressure
Hypopressives have traditionally been described as "low-pressure" exercises. However, emerging research is encouraging clinicians to think more broadly about posture, breathing and pressure organisation.
Saraiva S, McLean L. Hypopressive exercises do not cause transient changes in intra-abdominal pressure in females: an observational cohort study. International Continence Society Annual Meeting, 2024.
Birth trauma, levator avulsion and prolapse
Research continues to demonstrate associations between childbirth-related injury to the levator ani muscles, enlargement of the levator hiatus and pelvic organ prolapse.
Suggested search terms if you would like to explore this area further:
Levator ani avulsion and pelvic organ prolapse.
Levator hiatus dimensions and prolapse recurrence.
Vaginal birth and pelvic floor morphology.
Pelvic floor ultrasound and levator injury.
Additional themes explored in this article
The relationship between the diaphragm, abdominal wall and pelvic floor.
Pressure management during movement and exercise.
Menopause, collagen and connective tissue health.
The role of the nervous system, stress and protective muscle patterns in pelvic health.
As with all areas of women's health, the research is evolving. Anatomy, symptoms and recovery do not always correlate neatly, which is why treatment is rarely about one muscle, one exercise or one perfect solution.