Pelvic Floor Mapping: Redrawing the Forgotten Landscape
For many women, the pelvic floor feels like a mystery. We’re told to “squeeze it,” warned what happens if it doesn’t behave that we will be left with leaking, heaviness, prolapse, and a sense of fear with no real actual understanding.
Very few of us were ever taught how to actually sense, map, and connect with this part of our body.
That’s where pelvic floor mapping comes in.
Mapping is something quite exploratory and exciting discovering your body in a way you haven’t before. It isn’t about clenching. It’s about creating a sensory relationship, noticing, differentiating, and reclaiming your awareness. Like taking a blurred sketch and colouring it in with detail, curiosity, and real compassion.
"Touching your pelvic floor can be sensual, in the sense of awakening sensation, curiosity, and softness. That doesn’t mean it has to be sexual. You’re not aiming for arousal. You’re building a new sensory map, one that helps you feel safe, connected, and in tune with your body."
"When you practise pelvic floor mapping, you’re not just connecting to one muscle, you’re getting to know the whole tent. The fabric, the cords, the poles, the ground beneath it. And the more detailed your map, the more choice and confidence you have in how that tent supports you."
Hands-On Pelvic Floor Mapping
Adding the sense of touch to your awareness can be grounding and clarifying. This can be done through clothes, in a safe and comfortable way, so it feels less exposing.
One option is to place the palm or fingertips gently over the vulva (through leggings, pyjamas, or underwear) and simply notice:
warmth
pressure changes with breath
small movements in response to the diaphragm and pelvic floor
This turns something abstract into something tangible.
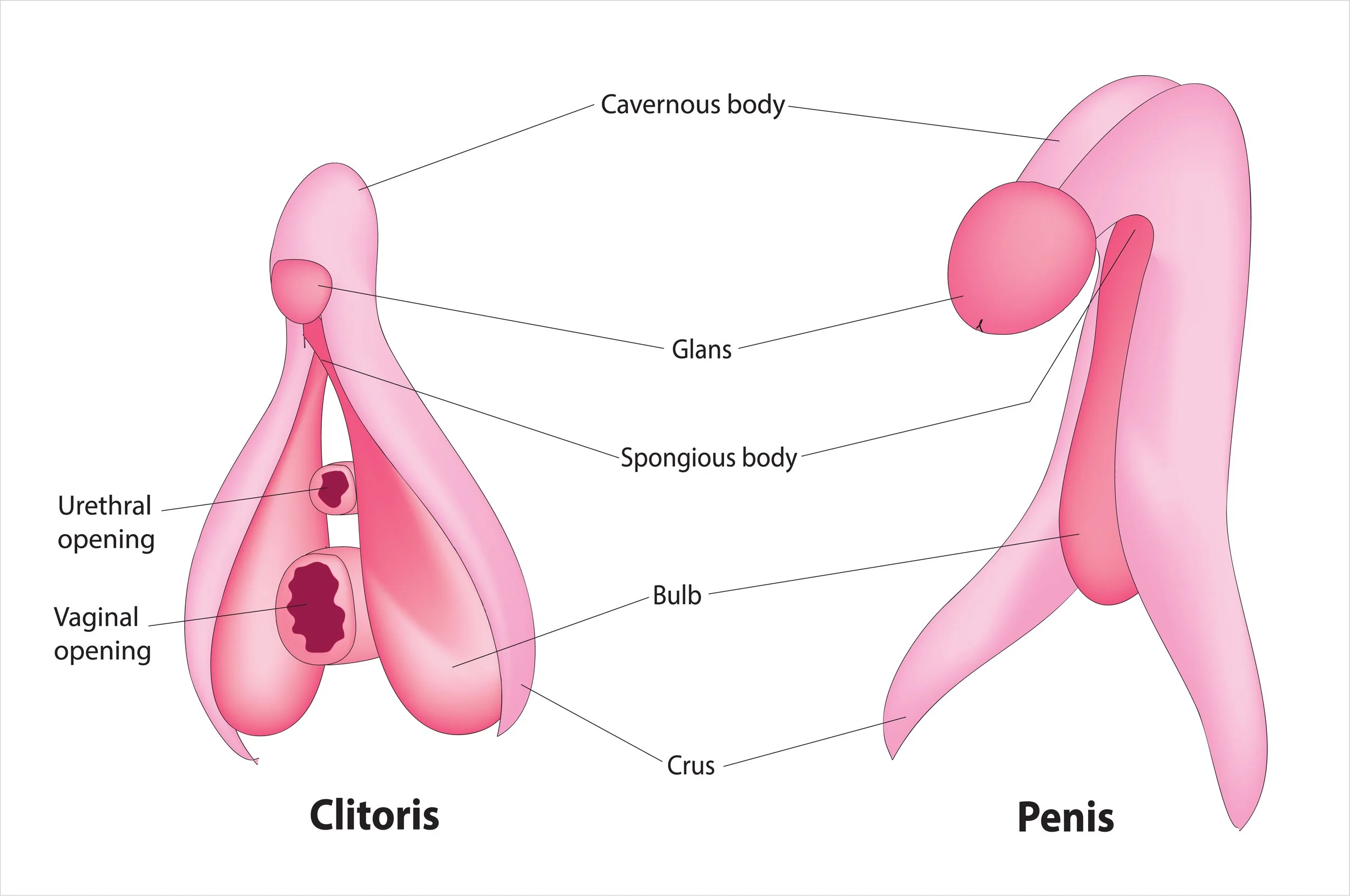
artists drawing of the anatomical clitoris and penis clinical image - in baby pink
Clitoral Nodding Awareness
The clitoris is more than the glans (the external part we see); it’s a large structure with legs (crura) and bulbs that anchor deep into the pelvis. It responds to pressure, breath, and subtle pelvic shifts.
A “clitoral nod” exercise could be:
Sit or lie in a comfortable position, hand resting gently over your vulva.
As you inhale, imagine your pelvic floor softening and the clitoris subtly moving downward/forward.
As you exhale, sense the pelvic floor recoiling and the clitoris gently lifting/backward — like a nod.
Do this slowly, like watching a flower bow and lift with the breeze.
This isn’t about sexual arousal, it’s more about learning that the clitoris is part of your pelvic floor map, not separate. The nod is often easier to sense than the deep hammock because it’s a tangible reference point.
Why This Matters
It helps us realise the pelvic floor is not invisible, it has a surface, an anchor, and a rhythm.
It brings safety and normalisation to touch, reclaiming the area as part of their whole body.
It can also reveal when there’s overactivity (if there’s no nodding or only tension).
Why Mapping Matters
When the pelvic floor is “off the map,” we often:
Grip and hold tension without realising.
Feel numb or disconnected after surgery, birth, or trauma.
Try endless Kegels but never feel results.
Mapping teaches us awareness and awareness gives choice. and choice can help us/you to restore confidence in our/your body.
Visualising the Pelvic Floor
Sometimes the easiest entry point is metaphor. These images give the nervous system a safe way to connect. Let’s dive into a few helpful ones. Don’t worry if they don’t all resonate with you. Metaphor is very subjective, perhaps with these as ideas you will develop one of your own and that is also perfect.
The Diamond
Your pelvic floor is like a diamond:
Pubic bone (front), tailbone (back), two sitting bones (sides).
Inhale: the diamond gently widens.
Exhale: the points draw softly to the centre.

Image of a diamond showing the tailbone, pubic bone and sit bones - pelvic floor mapping
The Hammock
Picture a hammock strung between your sitting bones.
Biomechanics show that on inhale, the rib cage expands, the sacrum tips slightly, and the sitting bones roll outward and upward.
Inhale: the hammock lengthens and lifts slightly, like a swing pulled taut.
Exhale: it recoils inward and returns to rest.
It’s not a sagging drop. It’s expansion and recoil, woven through bones, fascia, and breath.
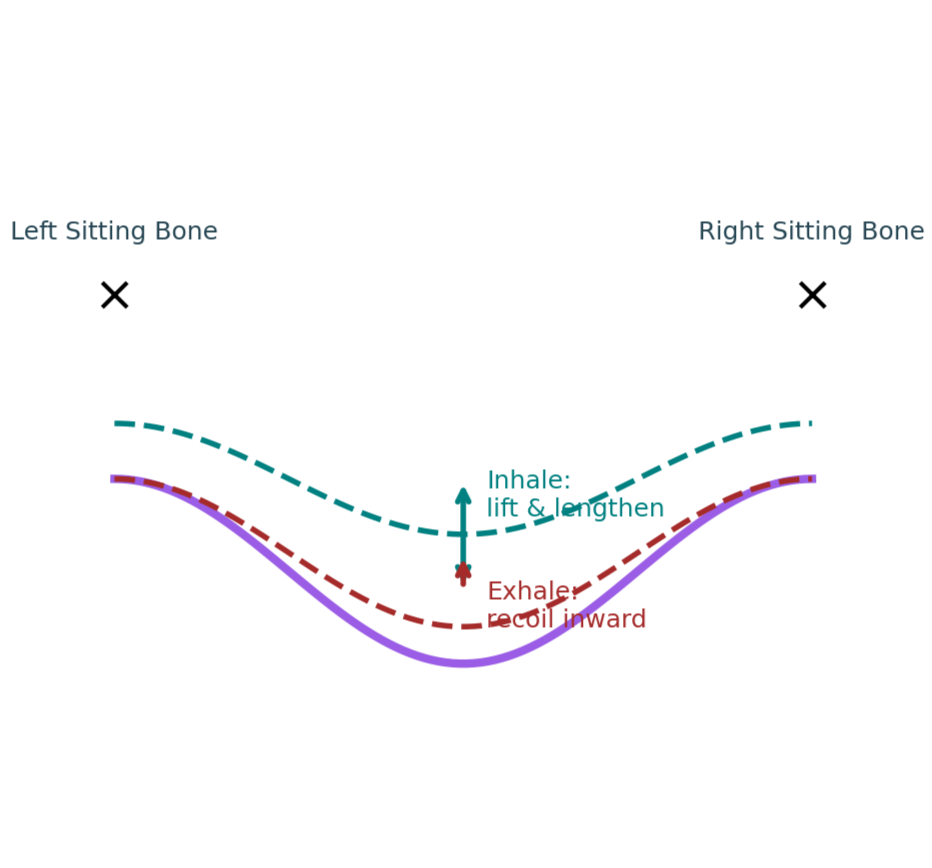
Image of a line drawing of the pelvic floor in its movement in inhale and exhale
Light Mapping
Imagine a warm light glowing in your pelvic bowl.
Let it spread through the whole base.
Notice where it shines bright and where it feels dim.
This simple scan reveals parts of your map that need attention.
Visual of light expanding
Hands-On Awareness: Sensual, Not Sexual
Sometimes mapping through touch helps. Place a hand over your vulva (through clothing is fine). Feel warmth, subtle shifts, even the tiny nod of the clitoris:
Inhale: a forward tilt.
Exhale: a gentle lift back.
This can feel sensual, but not sexual.
Sensual = tuning into sensation, warmth, rhythm.
Sexual = arousal and intimacy.
Mapping invites safe, sensual presence, without agenda.

Line drawing of a circle depicting the clitoris
“At rest, the vaginal walls lie softly together, held by fascial tone and natural pressure balance. But when that support system weakens, for instance after hysterectomy, birth, or long-standing downward pressure, the top of the vagina (the vault) can descend. It may feel more open, heavy, or as if something is sitting low. This isn’t failure, it’s feedback. The tissues are asking for new support and better pressure balance.”
Fine Mapping: The Calais Sequence
Once you’ve begun to sense the broad shapes of your pelvic floor with images like the Diamond or Hammock or one of your choosing, you can move into more detailed awareness. Blaise Germain Calais , a movement educator with a gift for anatomy and subtle sensing, described a sequence that helps us discover the different fibres and directions of the pelvic floor.
Think of it as learning to play piano scales instead of just pressing all the keys at once. Most pelvic floor exercises tell you to “squeeze everything.” Calais’ work invites you to explore which part you’re sensing, moving, and releasing. Try to only move the muscles and fascia being asked to move. Don’t use the glutes to activate the anus!
1. Urethra Awareness
Begin with your attention at the urethral opening (just above the vaginal entrance).
Imagine gently drawing this opening inward, as if you could lift it slightly toward the vulva.
Now visualise a thread pulling it upward to meet the bladder, then release.
Notice: can you feel a subtle lift and a soft letting go?
This helps you distinguish front-body awareness, a different sensation to the vagina or anus.
2. Vaginal Awareness
The vaginal canal is not one uniform space , it has front, back, sides, and depth.
Front to Back: Imagine the front wall of the vagina drawing toward the back wall. Then switch, the back wall moving toward the front. Repeat a few times.
Side to Side: Now sense the side walls moving inward, as if narrowing the space. Release.
String Bag Closure: Visualise the vagina like the opening of a drawstring bag:
Start low, near the vulva. Gently cinch inward, then release.
Move to the middle of the canal. Draw inward, then soften.
Finally, focus near the cervix at the top. Close, then open.
This practice helps you notice vertical differences (low, mid, high) as well as horizontal ones (front/back, side/side).
3. Anal Awareness
Bring your attention to the anus.
Draw in only the outer ring of muscle, the part you can consciously control.
Then soften fully, letting the tissue expand.
Keep the glutes, thighs, and tummy relaxed …no gripping or bracing.
The Key Principle
All of these micro-movements are small, subtle, and exploratory. They’re not about force, performance, or strength. They’re about clarity.
You may not feel all of them at first. That’s totally fine. The goal is not to achieve, but to notice, even the absence of sensation is part of your map. With time, awareness deepens and release becomes as reliable as contraction.
"Calais taught that the pelvic floor isn’t one lump to squeeze, but a landscape to explore. These subtle practices help you redraw the map, front and back, side to side, low, mid, and high, so that instead of a single on/off switch, you gain a whole keyboard of notes to play with."
What We Know - It is always a really good idea to ground our practical exploration in studies
1. MRI Imaging — They Move Together
Diaphragm and pelvic floor rise and fall in parallel, helping regulate pressure and spinal support.
Dynamic MRI studies show that the diaphragm and pelvic floor move in a synchronised rhythm. When the diaphragm descends, the pelvic floor lengthens slightly; when the diaphragm recoils upward, the pelvic floor is lifted by the organs in response.
This means the pelvic floor doesn’t act in isolation, it mirrors and complements the movement of the respiratory diaphragm, creating a pressure-regulating partnership that supports the organs and spine.
→ Source: dynamic MRI research on respiratory and pelvic motion in healthy women (J. Res. 2021).
2. Breathing Changes Pelvic Floor Length
Ultrasound shows inhale → lengthening; exhale → recoil. The pelvic floor breathes with you.
Ultrasound and biomechanical studies show that different phases of breath alter pelvic floor muscle length and tone. During inhalation, there’s a subtle lengthening and lateral expansion of the muscle fibres, and during exhalation a natural recoil or tension increase.
This variation demonstrates that the pelvic floor is responsive, not static, and directly influenced by respiratory rhythm, posture, and intra-abdominal pressure changes.
→ Source: comparative ultrasound and EMG data, 2018–2023 reviews on respiration–PFM interaction.
3. Fascial & Neural Synergy
They’re connected through fascia, nerves, and bone — a true full-body conversation.
It’s not only about muscles. The link between the diaphragm and pelvic floor travels through fascial continuities, nerve pathways, and bone mechanics.
The endothoracic fascia and endopelvic fascia form one continuous tension system connecting rib cage to pelvis.
Phrenic and pudendal nerves coordinate through spinal centres, creating reflexive movement patterns.
Subtle bone motions, like the sacrum tipping and ischial bones widening on inhalation, contribute to this synergy.
→ Source: biomechanical and neurofascial reviews (J Anat 2019; Clin Anat 2022).
4. Hypopressives Work Functionally
Clinical studies show improved tone, posture, and symptom relief via low-pressure breathing.
Clinical trials on Hypopressive exercise programmes report improvements in:
Pelvic floor muscle tone and endurance
Postural control and intra-abdominal pressure regulation
Reduction in symptoms of urinary incontinence and mild prolapse
The proposed mechanism is the rib cage expansion and apnoea hold, which creates a temporary drop in intra-abdominal pressure and a reflexive lift of the diaphragm and pelvic floor.
It’s not simply “strength training”, it’s a neuromechanical reset improving coordination and support.
→ Source: MDPI Applied Sciences 2024; Healthcare 2024 systematic reviews on Hypopressives.
5. Ongoing Research
3D imaging now quantifies micro-movements; consensus is clear, the pelvic floor breathes, it doesn’t drop.
“Every inhale and exhale invites movement through the pelvis.
The pelvic floor doesn’t drop; it breathes.”
Researchers are now using 3D ultrasound, MRI, and pressure sensors to quantify the exact millimetres of movement and tissue adaptation during Hypopressive and respiratory cycles.
While the overall picture supports a lift–lengthen dynamic, individual variation is huge, shaped by posture, breath habits, childbirth history, and fascial tension.
The emerging consensus: the pelvic floor is a living diaphragm within a multi-diaphragm system, dynamic, adaptive, and inseparable from breath.
→ Source: ongoing clinical imaging research (Pelvic Floor Centre Madrid, 2023–2025).
The difference between the larynx and uterus
Is the Vagina a Muscle?
“Contrary to how anatomy diagrams often look, the vagina isn’t a hollow tunnel waiting to be filled, it’s a soft, folded space with its walls gently resting together. At rest, it’s closed by nature, not by effort. This quiet closure comes from fascia, pressure balance, and subtle muscle tone, not from clenching. You don’t have to hold it shut, your body already knows how.”
A common myth: and one I totally thought was true!! “The vagina is a muscle.” it is so much more than that.
It isn’t. The vagina is a fibromuscular tube made of:
Fabric lining (mucosa) - Mucosal layer (innermost), this is the lining that keeps things moist, with folds (rugae) that let the vaginal canal expand and contract.
Elastic cords (smooth muscle)- Muscular layer, smooth (involuntary) muscle fibres that support the tone and elasticity of the vagina, also aiding in gentle contractile movement.
Anchoring ropes (fascia) - Adventitia / connective tissue layer, collagen, elastic fibres, fascia, and supportive connective tissue that attaches to surrounding pelvic walls and stabilises the vagina and uterus..
The squeeze you can feel comes from the muscles around it, not the wall itself.
Visualising the Vagina’s Structure
Imagine the vagina as a tent inside the pelvic bowl:
The fabric walls of the tent → this is the mucosal lining (soft, folded, moist, designed to expand and stretch).
The stretchy cords running through the fabric → this is the smooth muscle layer. They run in different directions, some around (circular) and some lengthwise (longitudinal) — giving the canal its ability to narrow, elongate, and tone. You don’t directly control these cords, but they respond reflexively (for example, during arousal, orgasm, or when something passes through).
The tent poles and ropes anchoring it to the ground → this is the fascia and connective tissue. They tether the vagina to the surrounding pelvic walls, linking it into the wider fascial web of the pelvis.
The ground beneath the tent → this is the pelvic floor muscles (levator ani, perineal muscles, etc.). These are under your conscious control, and when they contract or release, they change the shape and tone of the tent above.
So while the vagina itself isn’t “a muscle” you can flex at will, it’s part of a whole system of muscles, fascia, and connective tissue that makes it responsive, resilient, and alive.
The Tent Model
Visualise the vagina as a tent:
Fabric = lining
Cords = smooth muscle
Ropes = fascia
Ground = pelvic floor

Line drawing of the pelvis as a tent
Mapping isn’t about pulling one rope, it’s about understanding how the whole tent supports you.
🌙 Myth & Metaphor: The Tale of Vaginal Closure
There’s a story told in some traditions, that ancient women could consciously “seal” their vaginal canal all the way to the cervix during hunting or ritual, releasing it when safe.
No scientific evidence confirms this as literal fact.
But myths often carry symbolic truths, there is no smoke without fire! This one speaks to the body’s innate intelligence for closure and containment.
The Truth About Vaginal Closure
The vagina isn’t open or hollow however, it’s a potential space, its walls gently resting together at rest.
That quiet closure comes from:
Fascia providing tone and suspension,
Organ pressure balance between bladder and rectum,
Subtle resting muscle tone from the pelvic floor.
It’s softly closed, not clenched, like two silk petals gently touching.
When Support Changes — Understanding the Vaginal Vault
At the top of the vaginal canal sits the vault, the anchor point for fascial and ligamentous support.
When that system weakens, after childbirth, surgery, or prolonged downward pressure — the vault can descend, and the vaginal walls may lose their gentle contact.
This can feel like:
A sense of spaciousness or openness,
Loss of upward lift,
A heaviness or dragging near the pelvic floor.
Please don’t see a lack of any if these sensations as failure. They are a sign post and super valuable feedback feedback.. We need to notice before we can make change.
Through breath, fascial hydration, and posture, that support can be rebuilt.
The Symbolism Beneath the Story
Perhaps the myth wasn’t about closing the cervix at will, but about knowing when to contain and when to open.
Closure can be protective , not from fear, but from fullness.
It can mean drawing energy inward, claiming safety, and choosing where to direct attention.
“The pelvic bowl isn’t a void to be filled, but a centre of safety and sovereignty.”
Bringing It Together
Pelvic floor mapping isn’t about fixing or gripping.
It’s about curiosity, connection, and reclaiming the sensations and sensitivity in a positive way..
When you:
Visualise with Diamond, Hammock, and Light or your own one…
Touch with safety and sensual awareness,
Explore precision through Calais’ sequence,
Understand the tent-like anatomy,
Honour both biology and myth
You can absolutely redraw your map.
And when the map is clearer, you don’t just find muscles.
You find softness, strength, and belonging.
You find that your pelvic floor is a vital, reflexive, complex and sensual part of you and it’s simply waiting to be felt.
Next Step
If you’re ready to explore this for yourself, join my Beginner’s Hypopressives Programme (£29.95).
It’s designed to help you reconnect gently and safely starting with breath to begin your mapping
➡️ Join here